Le Infezioni in Medicina, n. 2, 191-197, 2026
doi: 10.53854/liim-3402-8
ORIGINAL ARTICLES
Insights into parvovirus B19 clinical and virological dynamics among blood donors
Massimo La Raja1, Nicola Benvenuto2, Monica Marconi1, Venera Costantino3, Anna Belgrano4, Stefano Di Bella5
1 Transfusion Medicine Unit, University Hospital of Trieste (ASUGI), Trieste, Italy;
2 Infectious Diseases Unit, University Hospital of Trieste (ASUGI), Trieste, Italy;
3 Microbiology Unit, University Hospital of Trieste (ASUGI), Trieste, Italy;
4 Clinical Laboratory Unit, University Hospital of Trieste (ASUGI), Trieste, Italy;
5 Clinical Department of Medical, Surgical and Health Sciences, University of Trieste, Trieste, Italy.
Article received 21 December 2025 and accepted 5 March 2026
Corresponding author
Stefano Di Bella
E-mail: stefano932@gmail.com
SUMMARY
Coinciding with the exceptional European resurgence of human parvovirus B19 (B19V), between 2023 and 2024, twelve B19V DNA-positive blood donations out of 27.737 were detected by the plasma fractionating industry via nucleic acid testing (NAT) and notified to the blood collection centers of Trieste and Gorizia (Italy).
In order to prevent potential B19V transmission, the implicated donors were recalled for clinical and virological follow-up for one year. None of the subjects had reported symptoms at the time of donation, though six subjects subsequently recalled either mild, transient symptoms in the days following donation or household exposure to fifth disease.
Index viral loads ranged from 6.6×105 to >1.0×109 IU/mL, with the majority of donations exceeding 106 IU/mL. The viral burden exhibited a rapid decline, dropping below 103 IU/mL after approximately four months and subsequently falling below 5×10³ IU/mL in all the monitored donors by eight months, although low-level viremia persisted. IgG antibodies were detected in all subsequent samples, while IgM persisted for up to 125 days in the majority of donors and remained detectable in three cases, including one instance lasting up to 355 days.
Since transfusion-transmitted B19V infection has been documented at viral loads as low as 5×10³ IU/mL, our data suggest that a theoretical risk of transmission may persist for up to nine months. Nevertheless, based on hemovigilance, transfusion-transmitted B19V infection appears to have limited clinical impact, likely due to the high level of population immunity and the predominance of non-infectious viral DNA during the late phase of infection. Overall, these observations support current policies that do not mandate routine B19V screening, while underscoring the importance of targeted testing in high-risk recipients and the temporary deferral of highly viraemic donors for 4–6 months.
Keywords: parvovirus B19, transfusion, blood donor, fifth disease, blood safety.
INTRODUCTION
B19V is a small non-enveloped DNA virus belonging to the family Parvoviridae, genus Erythroparvovirus [1, 2]. Its genome, which is approximately ~5.6 kb in size, encodes the nonstructural protein NS1 and two capsid proteins, VP1 and VP2. These proteins assemble into icosahedral particles of approximately 22–25 nm [3, 4]. B19V has been observed to have a marked tropism for human erythroid progenitor cells through its binding to the P blood group antigen (globoside), with additional co-receptors required for productive infection [1, 2]. This selective tropism is responsible for the profound hematologic effects of infection, particularly in individuals with increased red cell turnover or impaired immunity.
Transmission occurs mainly through respiratory droplets, but also via vertical transplacental passage, transfusion of blood or plasma-derived products, and organ or marrow transplantation [1, 5, 6]. Globally, B19V follows cyclical epidemics occurring at intervals of 3–5 years, typically peaking in late winter and spring. Seroprevalence increases with age, from approximately 15% in preschool children to over 80% in the elderly [1, 5]. Recently, several European countries reported an exceptional post-pandemic rebound in 2023–2024, with incidence rates far exceeding those observed during previous outbreaks [7-9].
The clinical spectrum of B19V infection is broad and depends heavily on the host. In immunocompetent children, it typically presents as erythema infectiosum (‘fifth disease’), characterised by a fever and the classic ‘slapped cheek’ rash [1, 10]. In adults, the condition may also manifest as an atypical rash, such as reticular exanthem [11]. In women, acute symmetric polyarthropathy is a frequent occurrence and may present with symptoms similar to those of rheumatoid arthritis [1, 4]. Patients with underlying hemolytic disorders are at risk of transient aplastic crisis, while immunocompromised individuals may develop persistent infection with pure red cell aplasia and chronic anemia [2, 12, 13]. It is estimated that in 30-50% of cases of primary maternal infection during pregnancy, there is a risk of vertical transmission, which can result in severe fetal anaemia, hydrops fetalis, or intrauterine death in up to 10% of cases. This risk is especially high when infection occurs in the second trimester [5, 6, 14, 15].
Of particular concern is the transfusion setting. Owing to its non-enveloped structure, B19V is highly resistant to standard viral inactivation procedures [1]. Asymptomatic donors have been shown to harbor extraordinarily high viral loads, with some cases exceeding 10¹² IU/mL, and such viremic donations may enter the blood supply [8]. Although transfusion-transmitted B19V infections are relatively rare, they can lead to severe complications in vulnerable populations, such as fetuses and immunocompromised or hematologically fragile recipients. Since 2008, United States Food and Drug Administration (FDA), followed by other associations such as the Plasma Protein Therapeutics Association (PPTA), have established an upper safety limit of 104 IU/mL for B19V DNA for plasma-derived medicinal products (PDMPs) [16, 17]. In the context of industrial screening, donations exceeding 106 IU/mL are typically identified and subsequently discarded. In such cases, the transfusion medicine services are notified. In the context of labile blood components (red blood cells and platelets), it is noteworthy that a limited number of European countries have adopted the B19V-DNA testing as a mandatory requirement for the qualification of blood products. In the remaining high-income countries, including Italy, there is a potential for the inadvertent transfusion of viraemic blood components from asymptomatic donors to patients.
Although the majority of infections are asymptomatic or self-limiting, B19V remains a clinically significant pathogen due to its hematologic impact, teratogenic potential, and resilience in the transfusion chain. These characteristics underscore the necessity for ongoing epidemiological surveillance and risk assessment, particularly in the domains of blood safety and maternal–fetal medicine.
Against this background, the present study aims to investigate for how long blood donors remain viraemic at potentially infectious levels after an acute B19V infection. By monitoring the kinetics of viral load and the dynamics of IgM/IgG seroconversion, we seek to define the time interval required for viral clearance below safety thresholds and thereby determine when donors can be safely reinstated for blood donation.
METHODS
This research was conducted at the Transfusion Medicine Department of the Azienda Sanitaria Universitaria Giuliano Isontina (ASUGI), which serves the provinces of Trieste and Gorizia in North-East Italy. The study retrospectively investigated the virological follow-up of all whole blood and plasma donors whose donations were notified by the PDMP pharmaceutical industry (CSL Behring) as B19V-DNA reactive. The study period extended from January 2023 to December 2024, coinciding with the exceptional European rebound outbreak of human B19V.
Eligible cases were defined as individuals who had previously donated blood and subsequently tested positive for B19V via NAT by the contracted plasma fractionator (CSL Behring). As part of the quality control process for the manufacture of PDMPs, plasma donations were screened in minipools of 96 samples using the cobas® DPX NAT assay (Roche Diagnostics; analytical sensitivity, 1334.4 IU/mL at pool level; detection limit for individual donations, 4.8×105 IU/mL). In instances where a pool was reactive, all constituent donations were subsequently resolved and quantified individually. Positive donations were excluded from fractionation, and the Transfusion Medicine Service was notified for donor recall and look-back. The delivery of notifications generally occurred within a timeframe of four to eight weeks subsequent to the donation of the index.
In accordance with Italian legislation all implicated donors were recalled and invited to undergo virological confirmation and subsequent follow-up. The quantitative detection of B19V-DNA was performed using the PVB19 Elite MGB® Kit. The results were expressed in copies/mL and converted to IU/mL according to the manufacturer’s conversion factor (1 copy = 0.5 IU) to ensure comparability with international standards. The presence of anti-B19V IgM and IgG antibodies was determined through the utilization of the LIAISON® Biotrin Parvovirus B19 IgM Plus and IgG Plus chemiluminescence immunoassays (DiaSorin). At the first control visit, donors were interviewed using a structured questionnaire that addressed recent exposure to exanthematous illnesses (e.g., fifth disease in children) and the occurrence of symptoms such as rash or flu-like illness around the time of the index donation (Figure 1).
Donors who were found to be DNA reactive at the initial control visit were scheduled for repeat NAT approximately three months later. The scheduling of subsequent appointments was adapted in accordance with the patient’s viral load dynamics and the availability of suitable donors.
The main retrospective objectives of the study were to describe the kinetics and duration of viremia and the time to clearance of IgM antibodies with persistence of IgG, and to verify retrospectively the clinical histories of donors the days around donation.
All data were anonymized and managed in compliance with Italian regulations for donor safety and privacy. The study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Trieste University Ethical Committee (protocol n° V8_240925). Written informed consent was obtained from all donors, as required by the Committee.
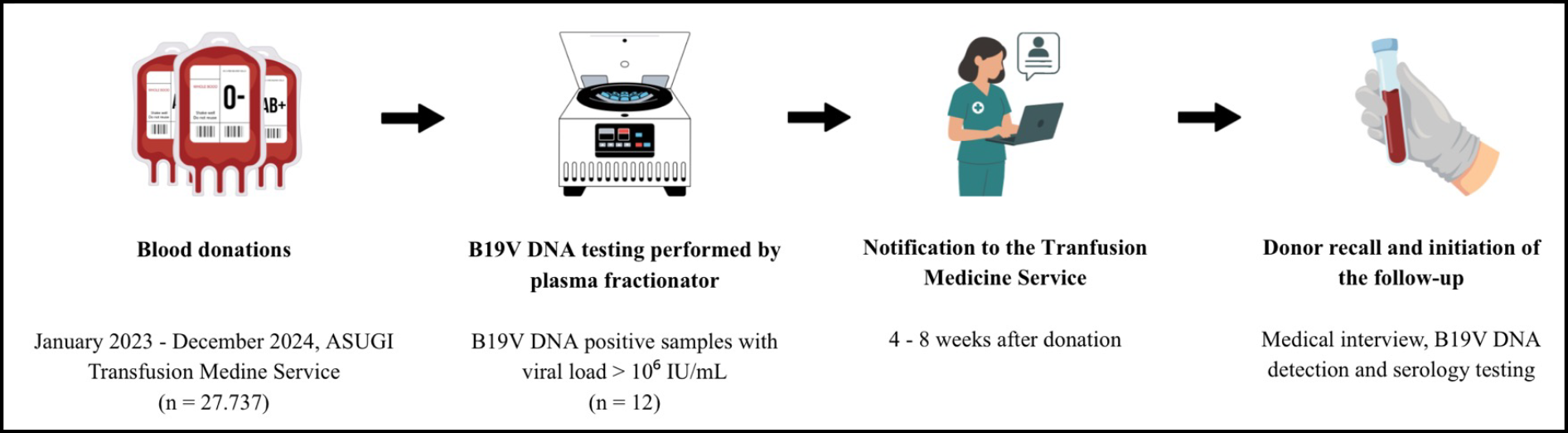
Figure 1 - Mean B19V viremia decay in blood donors.
RESULTS
Between January 2023 and December 2024, ASUGI blood collection centers received 27.737 blood donations; Among these, 11 whole blood donations and 1 plasma donation (12/27.737; 0.04%) were identified as B19V DNA–positive by the plasma fractionator’s industrial laboratory, and the corresponding donors underwent clinical evaluation and a virological follow-up.
None of the 12 donors had reported exposure to infectious diseases or the presence of symptoms at the time of donation, and no post-donation information indicating onset of illness was received. However, during subsequent follow-up interviews, 3 donors recalled contact with household cases of suspect fifth disease or other nonspecific exanthematous illnesses around the time of donation. Moreover, 3 donors reported the onset of mild symptoms in the period following donation. 2 donors experienced a pruritic skin rash, while 1 donor reported a febrile illness accompanied by a sore throat.
Index viral load data were available for all 12 donors. Titers ranged from 6.6×105 to >1.0×109 IU/mL, with a median of 8.55×106 IU/mL (IQR: 1.68×106–7.30×108 IU/mL). Furthermore, 10 donations exceeded 106 IU/mL. All donors were present for subsequent follow-ups, with the timing of these occurrences ranging from 49 to 156 days following the initial donation. This sequence is indicative of the scheduling of industrial notifications and the availability of donors. With regard to the number of follow-up visits, one donor had a single visit, five donors had two visits, and six donors completed three visits. The maximum period of observation for the final donor was 355 days.
Viral load findings are illustrated in Figure 2 and detailed Table 1. As anticipated, after the high-titer index donation, viral loads declined rapidly within the first month and then stabilized between 105 and 104 IU/mL through approximately the fourth month. Subsequent to this, all measured titers fell below 104 IU/mL. By approximately 8 months (≈244 days), all donors with available measurements consistently exhibited levels below < 5x103 IU/mL.
With respect to serologic evolution, the presence of IgG was identified in all subsequent samples. IgM were found to be present in all cases up to 125 days following donation. Thereafter, the presence of IgM was observed to disappear in nine donors, while it was found to persist in three cases, and in one case, up to 355 days.
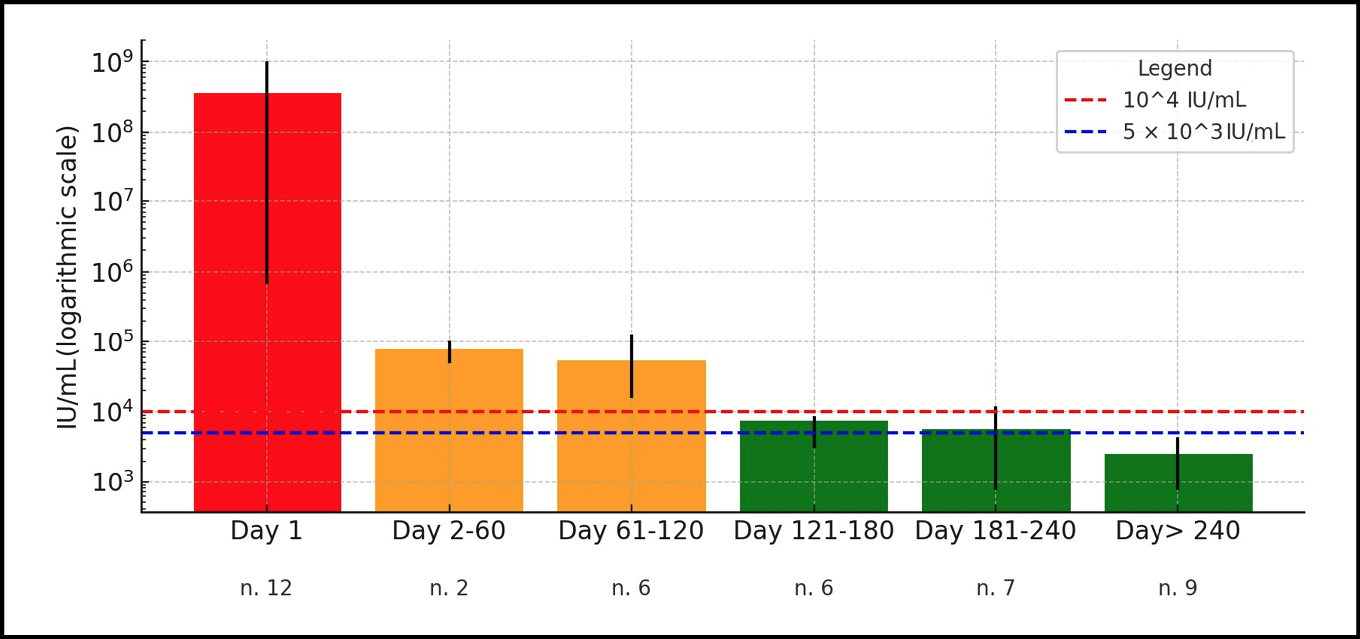
Figure 2 - Mean B19V viremia decay in blood donors.
Table 1 - Characteristics, medical history and viral load of the patients during the follow-up period.
|
Donation Time |
Gender/Age |
Medical History* |
Day 1 (IU/mL) |
Day 2-60 (IU/mL) |
Day 61-120 (IU/mL) |
Day 121-180 (IU/mL) |
Day 181-240 (IU/mL) |
Day 240-366 (IU/mL) |
|
May 2023 |
M 45 |
Contact |
1.6x106 |
8213 |
740 |
735 |
||
|
June 2023 |
M 29 |
Symptoms |
5.4x108 |
8735 |
5546 |
3218 |
||
|
June 2023 |
M 41 |
Negative |
1.2x107 |
8239 |
3623 |
1500 |
||
|
July 2023 |
M 38 |
Negative |
>1.0x109 |
123466§ |
6611 |
3729 |
||
|
January 2024 |
M 45 |
Negative |
5.1x106 |
8688§ |
7976 |
|||
|
April 2024 |
M 20 |
Negative |
>1.0x109 |
15593§ |
3097§ |
|||
|
April 2024 |
M 39 |
Contact and Symptoms |
6.4x108 |
49418§ |
2406§ |
|||
|
April 2024 |
M 58 |
Negative |
9.6x105 |
17126§ |
||||
|
May 2024 |
F 44 |
Negative |
3.7x106 |
48550§ |
4356 |
|||
|
May 2024 |
M 44 |
Negative |
1.7x106 |
41149§ |
1722 |
|||
|
May 2024 |
M 64 |
Contact |
6.6x105 |
103558§ |
6037 |
1743 |
||
|
June 2024 |
M 49 |
Symptoms |
>1.0x109 |
69804§ |
11885§ |
3042§ |
F: Female, M: Male.
*Contact: family contact with fifth disease or exanthematous disease; Symptoms: pruritic rash or sore throat around donation; Negative: non relevant history.
§Concomitant positive IgM.
DISCUSSION
An abnormal peak in B19V cases was also observed among blood donors in Trieste and Gorizia provinces (Italy) during 2023 and 2024. There were 12 notifications of B19 DNA-positive samples, equating to one every 2,311 donations, compared to none during the previous two years (2021–2022).
Our observations, based on a cohort of 12 donors, show that after the viraemic peak detected at the time of the index donation, the B19V viral burden declines rapidly but does not completely disappear in the following months. Instead, viremia reached a plateau in all cases, with moderately high and relatively stable viral loads (>5×10³ IU/mL) persisting for 5 to 8 months. Seroconversion, indicated by the absence of IgM antibodies, occurred after the 4th month, though not universally among all donors.
In consideration of the upper viral load limit currently accepted for plasma utilised in industrial fractionation (<104 IU/mL in the final pool), the findings of this study demonstrate that this threshold is consistently achieved after the fourth month following the initial donation, with a single exception extending up to 196 days [18, 19].
The viral burden threshold required to transmit B19V through labile blood products (red blood cells and platelets) remains a matter of debate [20, 21]. A previous study revealed that transmission can occur even at viral loads as low as 5×10³ IU/mL, particularly when the donor is IgM positive [22]. In the present cohort, viral loads did not consistently fall below this level until the 9th month after donation, indicating that the theoretical risk of transmission persists for several months even in the absence of symptoms.
Despite these observations and reports confirming the persistence of B19V-DNA in donor blood, the overall clinical impact of transfusion-transmitted B19V infection remains limited. Even during epidemic periods, up to 1% of blood donations may contain measurable B19V-DNA, yet no fatal transfusion-transmitted cases have been documented in the medical literature to date [23]. Moreover, no recent reports describe miscarriage or major fetal morbidity attributable to B19V transmission through transfusion in pregnant women.
This reassuring picture is likely explained by several factors. The majority of adults typically acquire immunity at an early stage in life, resulting in a low prevalence of susceptible individuals among transfusion recipients, who are predominantly elderly. Furthermore, experimental studies have demonstrated that approximately 5 months following infection, the presence of residual viral DNA in donor blood may signify non-infectious, capsid-deficient particles, likely neutralized by antibodies and incapable of replicating within target cells [21]. Despite the absence of in vivo studies to corroborate these findings, they may offer a potential explanation for the relatively minor clinical impact observed in transfusion-transmitted B19V infections, despite the frequent detection of viral DNA in blood products.
Collectively, these data lend support to the prevailing policy in the majority of high-income countries of refraining from implementing systematic B19V screening for blood donations [24]. Nevertheless, the implementation of targeted testing for high-risk recipients, including but not limited to immunocompromised patients, fetuses, and pregnant women, can be considered a rational precautionary measure. Indeed, certain European countries, including Germany and the Netherlands, have already adopted strategies to provide B19V-safe blood components through targeted screening or pathogen reduction protocols [25-27].
There are several limitations in our study. Overall, the number of cases was relatively small, 12 in two years, although this was an exceptional number, still it is limited compared with other larger studies [28]. Secondly, the scheduling of follow-up control visits and the number of these visits varied among donors. This variability was due to the fact that it reflected the level of donor interest in attending testing. The purpose of the control visits was to ensure that subsequent donations were B19-safe, a decision that depended on the donor’s availability and their willingness to donate further. In the initial follow-up visit, subjects were requested to recount anamnestic elements surrounding the donation time. This request was made at varying intervals, thereby introducing the possibility of recall bias. Moreover, the majority of labile products that were B19 DNA-positive were transfused outside the Department of ASUGI. Consequently, a comprehensive and detailed record review was not possible. However, neither the ASUGI Department nor other departments were notified of any clinically significant cases of B19 transmission.
CONCLUSIONS
In conclusion, the follow-up of B19V–positive blood donors identified during the 2023–2024 outbreak confirmed that viremia declines rapidly after the initial high-titer phase. However, the presence of viremia above 104 IU/mL persisted for a duration of several months, and in some cases up to eight months following the initial donation. Furthermore, the presence of IgM antibodies was observed to persist for a period of at least five months, subsequently undergoing a gradual decline. From a clinical and epidemiological perspective, although no symptoms were declared before donation, 3 out of 12 donors retrospectively recalled suggestive symptoms around the time of donation and other 3 donors recalled suspect B19V cases among family members.
The results emphasize the importance of coordinated communication and systematic follow-up between blood establishments and plasma fractionation industries to ensure optimal donor management and to monitor fluctuations in B19V circulation during epidemic peaks. Furthermore, selective screening of donations intended for high-risk recipients and the temporary deferral of donors with high viral loads for 4–6 months after detection may represent practical strategies to further minimize the risk of transfusion-transmitted B19V infection [29].
Funding
No funding was received for the preparation of this article.
Conflict of interest
The authors declare that there is no conflict of interest.
Acknowledgements
MLR conceived the idea of and designed the study; MLR, MM, VC and AB conducted data collection; MLR, NB and SDB analyzed the data; MLR and NB wrote the first draft; MLR, NB and SDB contributed to the interpretation of the data, writing and reviewing of the first draft of the manuscript. All authors reviewed and commented on subsequent versions of the manuscript. All authors approved the submitted version of the manuscript.
REFERENCES
[1] Broliden K, Tolfvenstam T, Norbeck O. Clinical aspects of parvovirus B19 infection. J Intern Med. 2006; 260: 285-304.
[2] Heegaard ED, Brown KE. Human parvovirus B19. Clin Microbiol Rev. 2002; 15: 485-505.
[3] Young NS, Brown KE. Parvovirus B19. N Engl J Med. 2004; 350: 586-597.
[4] Qiu J, Söderlund-Venermo M, Young NS. Human parvoviruses. Clin Microbiol Rev. 2017; 30: 43-113.
[5] Lamont RF, Sobel JD, Vaisbuch E, et al. Parvovirus B19 infection in human pregnancy. BJOG. 2011; 118: 175-186.
[6] Dittmer FP, Guimarães C de M, Peixoto AB, et al. Parvovirus B19 infection and pregnancy: Review of the current knowledge. J Pers Med. 2024; 14: 139.
[7] Farcet MR, Karbiener M, Aberham C, et al. Parvovirus B19 rebound outbreak 2024 and implications for blood- and plasma-product safety. Transfusion. 2024; 64: 2218-2221.
[8] Serricchio M, Gowland P, Widmer N, et al. Surveillance of blood donors detects an exceptional Parvovirus B19 outbreak in Switzerland in 2023/2024. Blood Transfus. 2025; 23(6): 515-522.
[9] European Centre for Disease Prevention and Control (ECDC). Risks posed by reported increased circulation of human parvovirus B19 in the EU/EEA. Available at: https://www.ecdc.europa.eu/en/publications-data/risks-posed-reported-increased-circulation-human-parvovirus-b19-eueea [accessed 4 September 2025]
[10] Bloise S, Cocchi E, Mambelli L, et al. Parvovirus B19 infection in children: a comprehensive review of clinical manifestations and management. Ital J Pediatr. 2024; 50: 261.
[11] Drago F, Ciccarese G, Broccolo F et al. Atypical exanthems associated with Parvovirus B19 (B19V) infection in children and adults. J Med Virol. 2015; 87(11): 1981-1984.
[12] Katoh D, Ochi Y, Hiramoto N, et al. Parvovirus B19 infection in adult patients after allogeneic stem cell transplantation: our experience of five cases and literature review. Bone Marrow Transplant. 2020; 55: 653-656.
[13] Holterhus M, Hennies M, Hillmann H, et al. Parvovirus B19 infection in pediatric allogeneic hematopoietic cell transplantation - Single-center experience and review. Transpl Infect Dis. 2023; 25: e14028.
[14] Kagan KO, Hoopmann M, Geipel A, et al. Prenatal parvovirus B19 infection. Arch Gynecol Obstet. 2024; 310: 2363-2371.
[15] Gigi CE, Anumba DOC. Parvovirus b19 infection in pregnancy - A review. Eur J Obstet Gynecol Reprod Biol. 2021; 264: 358-362.
[16] U.S. Food and Drug Administration (FDA). Nucleic Acid Testing to Reduce the Possible Risk of Parvovirus B19 Transmission by Plasma-Derived Products. Available at: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/nucleic-acid-testing-reduce-possible-risk-parvovirus-b19-transmission-plasma-derived-products [accessed 4 September 2025].
[17] Plasma Protein Therapeutics Association (PPTA). QSEAL NAT Testing Standard, v2.0. Available at: https://cdn.prod.website-files.com/638f893112c6eac0e46ac576/64517906a60bdb04ed8c3b74_NATTestingV2-3.pdf [accessed 3 September 2025].
[18] U.S. Food and Drug Administration (FDA). Guidance for Industry: Nucleic Acid Testing (NAT) to Reduce the Possible Risk of Parvovirus B19 Transmission by Plasma-derived Products, 2008. Available at: https://www.fda.gov/files/vaccines%2C%20blood%20%26%20biologics/published/Guidance-for-Industry---Nucleic-Acid-Testing--to-Reduce-the-Possible-Risk-of-Parvovirus-B19-Transmission-by-Plasma-Derived-Products.pdf [accessed 3 September 2025].
[19] Juhl D, Özdemir M, Dreier J, et al. Look-back study on recipients of Parvovirus B19 (B19V) DNA-positive blood components. Vox Sanguinis. 2015; 109: 305-311.
[20] Juhl D, Hennig H. Parvovirus B19: What Is the Relevance in Transfusion Medicine? Front Med. 2018; 5: 319619.
[21] Molenaar-de Backer MW, Russcher A, Kroes AC, et al. Detection of parvovirus B19 DNA in blood: Viruses or DNA remnants? J Clin Virol. 2016; 84: 19-23.
[22] Satake M, Hoshi Y, Taira R, et al. Symptomatic parvovirus B19 infection caused by blood component transfusion. Transfusion. 2011; 51: 1887–1895.
[23] Adamo MP, Blanco S, Viale F, et al. Human parvovirus B19 frequency among blood donors after an epidemic outbreak: relevance of the epidemiological scenario for transfusion medicine. Heliyon. 2020; 6: e03869.
[24] Styles CE, Hoad VC, Gorman E, et al. Modeling the parvovirus B19 blood safety risk in Australia. Transfusion. 2019; 59: 295-302.
[25] European Directorate for the Quality of Medicines & HealthCare (EDQM). Guide to the preparation, use and quality assurance of blood components. Available: https://www.edqm.eu/en/blood-guide [accessed 30 Oct 2025].
[26] Plümers R, Dreier J, Knabbe C, et al. Unexpected high incidence of parvovirus B19 nucleic acid detection in German blood donors in the winter/spring season 2023/2024. J Med Virol. 2024; 96: e29878.
[27] European Commission. Mapping more stringent blood donors testing requirements.Available at: https://health.ec.europa.eu/blood-tissues-cells-and-organs/blood/mapping-more-stringent-blood-donor-testing-requirements_en [accessed 3 September 2025].
[28] X. Wälti M, Natali M, Sanden A et al. Assessing B19V epidemiology and viremia dynamics in plasma donors: A comprehensive analysis. J Clin Virol. 2025; 181: 105873.
[29] Candura F, De Fulvio L, Massari MS et al. Comprehensive analysis of parvovirus B19 infection in blood donors: epidemiological trend and implications for transfusion safety and management strategies in Italy. Blood Transfus. 2025; 23(2): 168-175.