Le Infezioni in Medicina, n. 2, 177-190, 2026
doi: 10.53854/liim-3402-7
REVIEW
Sexually Transmitted Infections in adolescents and young adults: a growing public health challenge
Luca Pipitò1,2, Giulio D’Agati1,2, Antonio Cascio1,2
1 Department of Health Promotion, Mother and Child Care, Internal Medicine and Medical Specialties “G D’Alessandro”, University of Palermo, 90133 Palermo, Italy;
2 Infectious and Tropical Disease Unit, AOU Policlinico “P. Giaccone”, 90127 Palermo, Italy.
Article received 1 April 2026 and accepted 11 May 2026
Corresponding author
Antonio Cascio
E-mail: antonio.cascio03@unipa.it
SUMMARY
Background: Sexually transmitted infections (STIs) represent a major global public health challenge, particularly among adolescents and young adults aged 15–24 years, who account for a disproportionate share of incident infections worldwide.
Methods: We conducted a narrative review of the literature, synthesizing recent epidemiological data, risk factors, and prevention strategies related to STIs in adolescents and young adults. Relevant articles were identified through major scientific databases and international surveillance reports.
Results: This narrative review summarizes current epidemiological trends, risk factors, and prevention strategies related to STIs in young populations. The global burden of both bacterial infections, such as Chlamydia trachomatis, Neisseria gonorrhoeae, and Treponema pallidum, and viral infections, including HIV, human papillomavirus, and herpes simplex virus, remains high in this age group. Adolescents and young adults are particularly vulnerable due to a complex interaction of biological susceptibility, behavioral factors, and structural determinants such as limited access to sexual health services, stigma, and inadequate sexual health education. Specific subpopulations, including men who have sex with men, transgender youth, and young sex workers, experience markedly higher STI prevalence and incidence. A key challenge in STI control among young people is the high prevalence of asymptomatic infections, which substantially limits syndromic management and underscores the importance of systematic screening strategies. Evidence-based prevention approaches include vaccination, HIV pre-exposure prophylaxis, behavioral interventions, expanded screening programs, and youth-friendly healthcare services. Addressing the STI burden in young populations requires integrated public health strategies that combine biomedical interventions with efforts to reduce social and structural inequities influencing sexual health outcomes.
Conclusions: Reducing the burden of STIs in adolescents and young adults requires integrated, multi-level strategies combining prevention, early diagnosis, and equitable access to youth-friendly healthcare services, alongside targeted interventions addressing the specific needs of high-risk populations.
Keywords: Sexually transmitted infections, adolescents, young adults, sexual health, STI epidemiology, sexual risk behavior.
INTRODUCTION
Sexually Transmitted Infections (STIs) remain a major global public health concern, disproportionately affecting adolescents and young adults. According to the World Health Organization (WHO), more than 1 million curable STIs are acquired daily among individuals aged 15–49 years, with an estimated 374 million new cases of chlamydia, gonorrhea, syphilis, and trichomoniasis reported in 2020 [1]. In addition, viral STIs, including human immunodeficiency virus (HIV), human papillomavirus (HPV), and herpes simplex virus (HSV), persist as chronic or lifelong infections affecting hundreds of millions globally [2].
Individuals aged 15–24 years represent approximately 25% of the sexually active population but account for nearly 50% of newly acquired STIs worldwide, a pattern also observed in the United States [3]. Moreover, emerging infections such as mpox have further highlighted the potential for sexual transmission during outbreaks, with the 2022 epidemic disproportionately affecting young adult men, particularly men who have sex with men (MSM) [4].
The epidemiology of STIs in young populations is highly heterogeneous, reflecting differences in healthcare access, education, social determinants, and cultural contexts. The burden is greatest in sub-Saharan Africa, where adolescent girls and young women aged 15–24 years have substantially higher STI prevalence than males due to biological susceptibility and structural inequities [5]. In high-income countries, specific subpopulations such as migrants also experience a disproportionate STI burden. In Italy, surveillance data indicate that immigrant women have a significantly higher prevalence of Chlamydia trachomatis infection compared with native Italian women, particularly among young and pregnant women. Notably, a substantial proportion of infections in this population are asymptomatic, estimated at approximately 30–40%, with even higher rates reported among younger and pregnant individuals [6].
Globally, approximately one in four new HIV infections occurs among individuals aged 15–24 years, with especially high incidence among young women in sub-Saharan Africa; data from UNAIDS confirm that this population remains a key driver of ongoing HIV transmission worldwide [5].
In the United States, the STI burden is likewise concentrated among adolescents and young adults. Reported rates of chlamydia and gonorrhea peak among adolescent and young adult females, and many individuals acquire HPV during this developmental window. Early sexual debut further increases the risk of STI acquisition [7]. Certain adolescent subgroups are particularly vulnerable, including youth in detention facilities; those attending sexually transmitted disease (STD) clinics; adolescents involved in commercial sexual exploitation or survival sex; young males who have sex with males (YMSM); transgender youth; and adolescents with disabilities, substance misuse, or mental health disorders [7].
Heightened susceptibility during adolescence is multifactorial, reflecting interacting behavioral, social, and structural determinants such as multiple or concurrent partnerships, inconsistent barrier protection, lower socioeconomic status, and persistent barriers to healthcare access [7]. Beyond individual morbidity, the STI burden in this population also imposes substantial societal and economic costs through direct treatment expenditures, management of complications, productivity losses, and adverse mental health outcomes [7]. Key epidemiological indicators for STIs are summarized in Table 1.
Table 1 - Sexually transmitted infections burden across pathogens.
|
Infection |
Key epidemiological data |
|
Chlamydia trachomatis |
|
|
Neisseria gonorrhoeae |
|
|
Syphilis |
|
|
Mycoplasma genitalium |
|
|
HIV |
|
|
HSV-2 |
|
|
HPV |
|
|
Trichomonas vaginalis |
|
METHODS
This narrative review was conducted to provide a comprehensive overview of STIs in adolescents and young adults. A literature search was performed using major electronic databases, including PubMed, Scopus, and Web of Science. Additional sources included reports from international organizations such as the WHO, the Centers for Disease Control and Prevention (CDC), and the European Centre for Disease Prevention and Control (ECDC).
Keywords used in the search included “sexually transmitted infections”, “adolescents”, “young adults”, “chlamydia”, “gonorrhea”, “syphilis”, “mpox”, “HIV”, “HPV”, “HAV”, “Trichomonas vaginalis”, “vaginosis” and “prevention”. Articles were selected based on relevance to epidemiology, risk factors, and prevention strategies in young populations. Both observational studies and systematic reviews were considered.
Given the narrative nature of this review, no formal systematic review protocol or meta-analysis was performed.
RESULTS
Specific sexually transmitted infections: burden and distribution
Bacterial STIs: Chlamydia, Gonorrhea, Syphilis, and Mycoplasma genitalium
Chlamydia trachomatis remains one of the most prevalent bacterial STIs globally, with the highest burden among individuals aged 15–24 years, where prevalence ranges from 3% to 10% depending on region [8]. Globally, pooled prevalence estimates (2009–2016) were 3.8% in women and 2.7% in men aged 15–49 years, with incidence in 2016 of 34 cases per 1,000 women and 33 per 1,000 men [9]. The number of sexual partners was associated with the seroprevalence of C. trachomatis among HIV positive women in Nigeria [10].
The significance of chlamydia extends beyond acute infection, as untreated and often asymptomatic infections lead to serious sequelae [11]. Evidence summaries indicate that approximately 17.1% of women with untreated chlamydia infections experience pelvic inflammatory disease, with salpingitis occurring in 7.3% of cases, and long-term reproductive consequences, including tubal factor infertility, affecting approximately 29% of cases [12]. In addition, C. trachomatis has evolved mechanisms of immune evasion that allow persistent infection within host cells. This chronic persistence can trigger sustained inflammatory responses, contributing to tissue damage and long-term complications. Emerging evidence also suggests a potential role in carcinogenesis, particularly in the presence of co-infections such as HPV and HIV, with studies indicating possible associations with cervical and ovarian cancers [13]. Although less common than in females, accumulating evidence links C. trachomatis to impaired male fertility through obstruction or dysfunction of the epididymis, direct sperm damage, and inflammatory alterations of seminal parameters. Recent meta-analyses show a significant association between infection and infertility (Odd Ratio [OR] = 3.68 in case-control studies) [14].
Lymphogranuloma venereum (LGV), caused by invasive C. trachomatis serovars (L1-L3), has re-emerged in Europe, with over 3,000 cases reported in the EU/EEA in 2023. It predominantly affects MSM, often with HIV co-infection, though increasing cases in HIV-negative individuals suggest broader transmission [15]. Most cases occur in adults aged 25-44 years (peak 25-34), with anorectal involvement predominating. Untreated LGV may cause severe complications, including proctocolitis, fibrosis, strictures, fistulae, and genital elephantiasis, while asymptomatic rectal infection is common, especially in MSM [15, 16].
Neisseria gonorrhoeae has an increasing global incidence, particularly among young people.
Global prevalence is estimated at 0.7% in men and 0.9% in women, with incidence in 2020 of 19 cases per 1,000 women and 23 per 1,000 men aged 15-49 years [9]. In the United States, rates declined slightly in 2022-2023 (179.5 cases per 100,000; 601,319 cases), but remain highest among individuals aged 19-24 years and Black populations. In Europe, the highest notification rates occur among 20–24-year-olds (99.6/100,000 men; 48.1/100,000 women) [17].
The rise in gonorrhea incidence is particularly alarming given emerging resistance to antimicrobial treatments, which threatens the effectiveness of current standard therapeutic regimens and the necessity of effective management strategies to prevent severe consequences, such as infertility and pelvic inflammatory disease, which can result from delayed intervention in young women.
Recent data indicate increasing resistance to extended-spectrum cephalosporins, including ceftriaxone and cefixime, in several countries between 2022 and 2024, including Europe and the USA. In addition, resistance to ciprofloxacin has reached extremely high levels, approaching 95% in some settings [18].
An additional emerging concern is oropharyngeal gonorrhea, particularly among MSM. Pharyngeal infections are frequently asymptomatic and therefore often remain undiagnosed, contributing to ongoing transmission. The introduction of nucleic acid amplification tests (NAATs) has significantly improved detection rates at extragenital sites, revealing a higher burden of pharyngeal and rectal infections than previously recognized [19]. These anatomical reservoirs are also considered important in the development and spread of antimicrobial resistance.
Syphilis has resurged globally, with approximately 8 million new cases annually among individuals aged 15-49 years [20]. In 2016, global prevalence was 0.5% in both sexes (≈19 million cases), with an incidence of 1.7 and 1.6 per 1,000 women and men, respectively [9].
Adolescents and young adults remain significantly affected: in the United States, individuals aged 15–24 years account for nearly half of cases, while in Europe approximately 11% occur in this age group, with rising trends and higher rates in men (up to eightfold), particularly those aged 25-34 years [8, 21]. Early syphilis (primary, secondary, and early latent) represents the most infectious stage. Secondary syphilis can present with a wide spectrum of cutaneous lesions, including psoriatic-like, verruciform, and ulceronodular lesions that are often variable and atypical, which may lead to missed or delayed diagnosis. If untreated, this can result in serious complications, including ocular involvement, central nervous system manifestations, and late-stage sequelae such as gummatous lesions, tabes dorsalis, paresis, and cardiovascular involvement [22-28]. Latent syphilis, which is asymptomatic, represents a substantial proportion of cases in Italy and has been reported to have a higher prevalence in individuals with HIV infection [29].
Mycoplasma genitalium is an emerging STI with a prevalence of 1-2% in the general population, primarily affecting young adults, but reaching 3–10% or higher in high-risk groups [30]. Infection is frequently asymptomatic, particularly in women, facilitating transmission. It is associated with cervicitis and pelvic inflammatory disease, with potential reproductive consequences [31]. Diagnosis relies on NAATs, as culture is rarely feasible; however, routine screening in asymptomatic adolescents is not recommended due to limited evidence and increasing macrolide and fluoroquinolone resistance [7, 32].
Viral STIs: HIV, HSV, HPV, HAV, and MPOX
Young people remain disproportionately affected by the global HIV epidemic. In 2024, an estimated 0.7% of adults aged 15-49 years were living with HIV, with women and girls representing 53% of cases. Approximately 1.3 million new infections occurred globally, with a substantial proportion among adolescents and young adults (15-24 years). Adolescent girls and young women bear a particularly high burden, with ~210,000 new infections in 2023 and ~4,000 new infections weekly, mainly in sub-Saharan Africa [5]. Key populations, including MSM, sex workers, people who inject drugs, and transgender individuals, account for most new infections in many regions, with additional risk linked to recreational drug use and unprotected anal intercourse among young MSM [33]. In Europe, individuals aged 15-29 years represent a significant proportion of new diagnoses [34].
A global meta-analysis of people who inject drugs reported a pooled HIV incidence of 1.7 per 100 person-years, with young individuals (≤25 years) having a 50% higher acquisition risk compared with older adults [35]. Similarly, a meta-analysis in young women engaged in sex work found higher HIV incidence in younger versus older women (5.3 vs 2.8 per 100 person-years) and very high pooled prevalence among those initiating sex work before age 18 (28.8%) [36]. The global epidemiology of HIV demonstrates that adolescent girls aged 15-24 years in sub-Saharan Africa experience infection rates eight times higher than their male peers, highlighting the intersection of biological vulnerability and social-structural inequities [37]. Furthermore, reports of advanced HIV disease showed high prevalence (46.7%) in young people with HIV in some regions of sub-Saharan Africa [38]. Additional systematic reviews confirm important gaps in testing coverage: a 2025 meta-analysis of adolescents and young adults reported a pooled HIV testing rate of only 32%, underscoring ongoing diagnostic gaps in youth populations [39].
Herpes simplex virus type 2 (HSV-2) affects an estimated 491 million individuals aged 15-49 years globally, with incidence peaking soon after sexual debut and strongly associated with sexual behavior and key population status [40]. The high prevalence of HSV-2 is particularly significant because of its role as a cofactor in HIV acquisition and transmission, up to threefold higher [41].
HSV-1 is increasingly recognized as a cause of genital herpes, particularly in younger populations. In 2020, an estimated 16.8 million new genital HSV-1 infections occurred globally, with the highest incidence in young individuals and women [42]. HSV-1 now accounts for ~34% of genital herpes overall and nearly 50% of first episodes, reflecting declining childhood exposure and increased susceptibility at sexual debut [43]. Primary infection typically occurs in young adults (median age ~26 years) and is associated with early genital viral shedding and transmission potential [44]. Primary infection may present with a systemic febrile illness accompanied by extremely painful mucocutaneous lesions that can extend to the perigenital area. Viral dissemination may be facilitated by shaving or other forms of local skin microtrauma, which can promote autoinoculation and lesion spread [45].
Human papillomavirus (HPV) remains highly prevalent among adolescents and young adults, with an estimated prevalence of 32.8% in individuals aged 15-24 years and peak acquisition occurring shortly after sexual debut [46].
Younger males (≤20 years) may exhibit particularly high rates of multiple infections (~49.3%) [47]. Globally, nearly one in three men carries at least one HPV type, and one in five harbors high-risk types, underscoring their role as an important virological reservoir [48]. Population-based data indicate comparable or higher HPV prevalence in men than in women (41.8% vs 38.4% for any HPV; 24.2% vs 19.9% for high-risk types), as well as a higher prevalence of oral HPV infection in men (9.1% vs 4.6%) [46, 49]. High-risk HPV prevalence remains substantial in young cohorts, including 38% in southern Italy [49].
Persistent infection with high-risk HPV types is causally associated with more than 95% of cervical cancers and a significant proportion of other anogenital and oropharyngeal malignancies, with HPV-16 and HPV-18 accounting for the majority of cases [46, 50]. The highest cervical HPV prevalence is observed in regions such as sub-Saharan Africa (approximately 24%), particularly among women younger than 25 years [46, 51].
Hepatitis A virus (HAV), traditionally transmitted via the fecal–oral route, is increasingly recognized as an STI among MSM, primarily through oro-anal contact [7, 52]. Disease severity increases with age, with ~70% of adults developing symptomatic infection [7].
Recent outbreaks in high-income countries have disproportionately affected young adult MSM, including a ~294% increase in U.S. incidence (2016-2018) and outbreaks across Europe, including ~1,400 MSM-associated cases and a large Italian outbreak (513 cases) [52, 53]. Molecular analyses identified co-circulating genotype IA strains with evidence of intercontinental spread linked to international travel and interconnected sexual networks [51].
The 2022–2024 mpox outbreak (clade IIb, lineage B.1) marked a shift toward predominantly sexual transmission, particularly among MSM. Over 100,000 cases have been reported globally, with transmission linked to close physical and sexual contact, including condomless receptive anal intercourse (adjusted OR ~5.4) [54]. American CDC data further indicate that sexual exposure is a key driver of infection, with significantly increased risk associated with condomless receptive anal intercourse (adjusted OR ≈ 5.4) among sexually active individuals aged 18-49 years [55]. Cases have primarily involved young and middle-aged adults, while adolescents (<18 years) accounted for only ~1% of infections, indicating concentration within adult sexual networks [55, 56].
Trichomonas vaginalis and Bacterial Vaginosis
Trichomonas vaginalis is likely the most common non-viral STI worldwide, with an estimated 276 million new cases annually [57]. Prevalence is highest among women, ranging from 5% to >20% in some populations, with global estimates of 5.3% in women and 0.6% in men aged 15–49 years. Incidence is estimated at 40 per 1,000 women and 42 per 1,000 men [9].
A major challenge in control is the high proportion of asymptomatic infections in both sexes, facilitating ongoing transmission [57]. Infection is associated with reproductive tract inflammation (vaginitis, cervicitis, urethritis), adverse pregnancy outcomes (preterm birth, low birth weight, premature rupture of membranes), and increased susceptibility to HIV and HSV-2. Treatment reduces HIV genital shedding in co-infected individuals. Epidemiological evidence also suggests an association with cervical neoplasia (≈1.9-fold increased risk) and a possible, though inconsistent, link with prostate cancer [57].
Although bacterial vaginosis (BV) is not formally classified as an STI, substantial epidemiological and microbiological evidence indicates a strong association with sexual activity and increased risk of STI acquisition [58]. It is the most common cause of vaginal dysbiosis in reproductive-age women and is characterized by depletion of Lactobacillus species and overgrowth of anaerobes such as Gardnerella vaginalis, leading to altered vaginal pH and impaired mucosal defenses [58]. Transmission dynamics are influenced by penetrative and non-penetrative sexual contact, including oro-genital exposure [59]. Risk factors include smoking, douching, multiple partners, sex toy use, intrauterine contraception, antibiotic exposure, substance use, and partner-related factors [60].
BV is associated with approximately 1.8–1.9-fold increased risk of acquiring STIs such as C. trachomatis and N. gonorrhoeae [61]. A randomized controlled trial demonstrated that partner treatment significantly reduces recurrence (35% vs 63% at 12 weeks), supporting the role of sexual partners as reservoirs [62]. Given its high prevalence in adolescents and its role as a cofactor for STI transmission, early recognition and management, including consideration of partner treatment, may be important for comprehensive STI prevention strategies.
Risk factors and vulnerable populations
Behavioral and Demographic Risk Factors and Social Determinants
Sexual risk behaviors remain the primary drivers of STI acquisition in adolescents, including early sexual debut, inconsistent condom use, multiple or concurrent partners, and limited sexual health knowledge [2].
Recent surveillance data indicate concerning trends in protective behaviors among adolescents. A large international study from the WHO Health Behaviour in School-aged Children survey reported a decline in condom use among sexually active adolescents between 2014 and 2022, with nearly 30% of adolescents reporting no condom or contraceptive use during their last sexual intercourse, increasing transmission risk [63]. Substance use is a major determinant, with illicit drug use associated with more than threefold higher STI risk (aOR 3.10), and delinquent behavior also increasing risk (aOR 2.31) [64]. Notably, chemsex is strongly associated with STI acquisition, particularly among MSM and young adults, with prevalence up to 33.8% in STI clinic populations and increased odds of syphilis (OR 1.74), gonorrhea (OR 1.78), and chlamydia (OR 1.43) [65, 66].
Demographic characteristics also influence STI risk within the youth population. Age gradients have been observed even within the typical high-risk group of 15-24-year-olds. Young adults aged 22-25 years demonstrate modestly higher odds of STI acquisition compared with those aged 18-21 years (aOR 1.26; 95% CI 1.12-1.42), possibly reflecting increased sexual network size and cumulative exposure over time [64].
Partnership status also influences risk, with higher odds among unmarried individuals (aOR 1.29) and, especially, among separated/divorced individuals (aOR 1.93), consistent with increased partner turnover and concurrency [64].
Structural determinants, including socioeconomic status, healthcare access, stigma, and limited sexual health literacy, contribute to delayed diagnosis and ongoing transmission [67]. Beyond traditional demographic variables, emerging evidence suggests that mental health and psychosocial vulnerability may further increase susceptibility to STIs in young populations. A large nationwide cohort study published in 2024 found that adolescents and young adults with borderline personality disorder had a markedly elevated risk of STI diagnosis compared with matched controls, highlighting the role of impulsivity, emotional dysregulation, and associated high-risk behaviors in shaping sexual health outcomes [68].
Sexual network dynamics, including partner concurrency and assortative mixing, are critical determinants of transmission. Increasing use of digital platforms and geosocial applications is associated with higher partner numbers and condomless sex, although these tools also offer opportunities for interventions such as digital partner notification and targeted prevention [69].
Racial and ethnic disparities
Substantial racial and ethnic disparities persist, driven by structural inequities and differences in access to care. In the United States, non-Hispanic Black adolescents and young adults have significantly higher STI risk (aOR ~1.7–1.8 vs White youth), even after adjustment for behavioral factors [64].
Surveillance data show markedly higher chlamydia rates among Black adolescents, with incidence in females aged 15–19 exceeding 6,800 per 100,000 compared with ~1,500 in White females, and rates among Black males more than ninefold higher than in White males. Similar disparities are observed for gonorrhea and syphilis [70].
Differences in healthcare access further contribute to disparities: Black youth are less likely to receive testing in primary care settings and more likely to be tested in emergency departments, reflecting inequities in preventive care access [71].
Gender and Sexual Minority Populations
Transgender and gender minority youth (TGMY) represent a highly vulnerable but understudied population. In a U.S. multicenter cohort (aged 16-24 years), approximately one-third reported a lifetime history of non-HIV STIs, most commonly chlamydia (55%), syphilis (48%), and gonorrhea (47%) [72]. Transfeminine youth assigned male sex at birth demonstrated more than fourfold higher odds of STI diagnosis compared with transmasculine youth assigned female sex at birth (OR 4.06), while individuals identifying as nonbinary also showed significantly elevated STI risk, see Figure 1 [72]. Structural barriers, including limited access to gender-affirming care, stigma, and lack of tailored education, along with factors such as transactional sex and housing instability, contribute to increased vulnerability [73].
MSM similarly experience high STI burden, with incidence rates in PrEP cohorts ranging from 1.8-14.9 per 100 person-years for syphilis, 13.3-43 for gonorrhea, and 15.1-48.5 for chlamydia [74]. Adolescent female sex workers represent another high-risk group, with studies reporting up to 56.7% co-infection with multiple STI pathogens [75, 76].
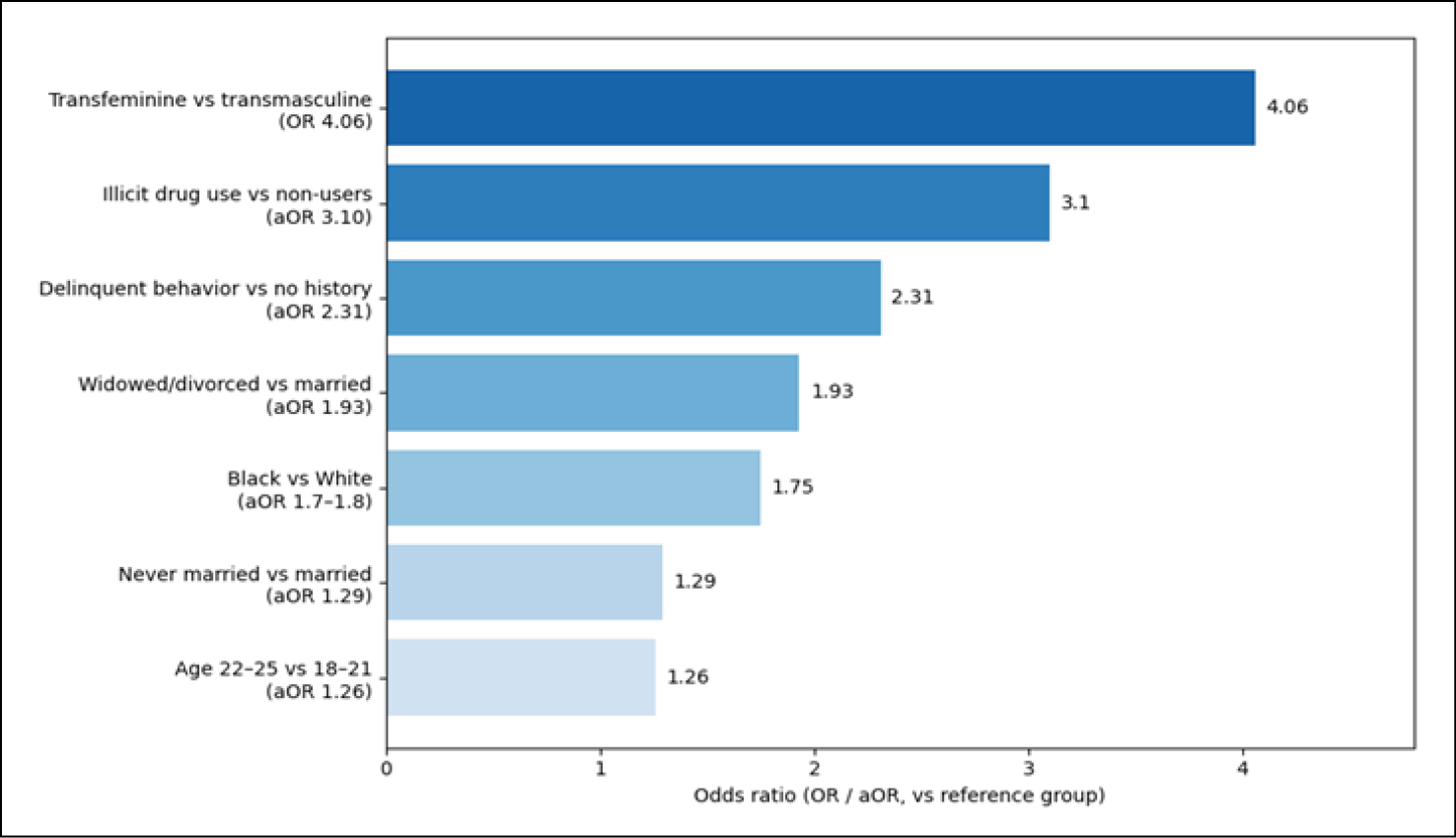
Figure 1 - Risk factors in young adults associated with sexually transmitted infection acquisition.
Epidemiology of asymptomatic infections and screening implications
A major challenge in STI control among adolescents is the high prevalence of asymptomatic infections, limiting the effectiveness of syndromic management. Common STIs, including C. trachomatis, N. gonorrhoeae, M. genitalium, and T. vaginalis, are frequently asymptomatic, particularly in younger populations [11]. Population-based data highlights the magnitude of this issue. In a South African study, laboratory testing identified infections in 70.2% of young women and 10.4% of men, while only 16.2% of women reported symptoms, and nearly all infected men were asymptomatic. Symptom-based detection showed extremely low sensitivity (~14% in females, 0% in males) [77]. Chlamydia exemplifies this pattern, with 70–90% of infections in women and up to 50% in men asymptomatic, facilitating ongoing transmission and long-term complications [7, 11]. Similar recommendations have been adopted in European and WHO guidelines, emphasizing the use of NAATs due to their superior sensitivity and ability to detect infections at multiple anatomical sites.
Prevention Strategies: Current Evidence and Effectiveness
Vaccination
Vaccination represents one of the most effective strategies for preventing STIs among adolescents and young adults. HPV vaccination has demonstrated very high efficacy in preventing infection with vaccine-targeted HPV types, reaching ≥90% protection among individuals vaccinated prior to viral exposure [78]. The quadrivalent HPV vaccine, targeting HPV types 6, 11, 16, and 18, has been shown to reduce the incidence of genital warts by approximately 83% and cervical or vulvar intraepithelial neoplasia by 78% [78].
Current immunization guidelines recommend routine HPV vaccination for adolescents aged 11–12 years, with vaccination possible starting at age 9 years and catch-up vaccination recommended through age 26 years for individuals not previously vaccinated [79]. For adults aged 27–45 years, vaccination may still provide benefit in selected cases and is therefore recommended based on shared clinical decision-making between patients and healthcare providers [79].
In addition to routine vaccination strategies, increasing attention has been directed toward developing targeted programs for individuals who were not vaccinated in earlier cohorts. These include catch-up vaccination campaigns and the implementation of network-based models to improve vaccine uptake, particularly among adolescents and young adults who missed routine immunization [80]. Effective communication strategies also play a critical role in improving HPV vaccine acceptance. Evidence suggests that tailored messaging, the use of trusted healthcare providers as messengers, and culturally sensitive communication approaches significantly enhance vaccine uptake [81].
Despite the strong evidence supporting HPV vaccination, global vaccine coverage remains uneven. Between 2006 and 2014, HPV vaccination programs expanded substantially but were primarily implemented in high-income and upper-middle-income countries, while low-income countries, where the burden of cervical cancer is highest, have experienced limited vaccine access [82]. Global estimates indicate that fewer than 20% of girls worldwide have received the full HPV vaccine series, highlighting major inequities in prevention efforts [48].
In addition to HPV vaccination, hepatitis B vaccination remains a key strategy for preventing sexually transmitted HBV infection and its long-term complications, including chronic hepatitis and hepatocellular carcinoma. Universal childhood vaccination programs have markedly reduced incidence in vaccinated cohorts [83].
Hepatitis A vaccination is also recommended for high-risk populations, particularly men who have sex with men, and has proven effective in reducing outbreak-related transmission and disease burden [84].
However, susceptibility remains high, with approximately 74% of U.S. adults ≥20 years lacking protective antibodies and low vaccine coverage among MSM (25-45%) [85].
Meningococcal B vaccines may confer partial cross-protection against N. gonorrhoeae. A pooled analysis of available observational studies suggests approximately 32.4% effectiveness against gonorrhea acquisition after a single vaccine dose [86], supporting the hypothesis that shared antigenic structures between N. meningitidis and N. gonorrhoeae may induce cross-reactive immune responses [87].
Current strategies to mpox prevention rely on smallpox-derived vaccines, including ACAM2000, MVA-BN (Imvanex®/Jynneos®/Imvamune®), and LC16m8 [4]. MVA-BN is preferred due to its favorable safety profile and is recommended for pre- and post-exposure prophylaxis; while it may not fully prevent infection, it reduces disease severity and transmission. Immunogenicity studies show strong neutralizing responses after two doses, though waning immunity may necessitate boosters. In contrast, ACAM2000 is associated with a higher risk of adverse events, and LC16m8, while promising, faces logistical limitations [4].
Pre-exposure Prophylaxis for HIV and other STIs
Pre-exposure prophylaxis (PrEP) is a highly effective HIV prevention strategy. The iPrEx trial demonstrated that daily oral tenofovir disoproxil fumarate/emtricitabine (TDF-FTC) reduced HIV acquisition by 44%, with >90% efficacy among adherent individuals [88].
Event-driven (“on-demand”) PrEP, as shown in the IPERGAY trial, reduced incidence by ~86% among MSM [89].
Despite strong clinical evidence, PrEP uptake remains suboptimal, particularly among populations experiencing the highest HIV burden. Barriers to PrEP use include limited awareness, perceived low personal risk, stigma from healthcare providers or peers, cost concerns, and distrust of healthcare systems [90]. These barriers are especially relevant for adolescents and young adults, who may face additional challenges such as limited access to confidential healthcare services and insurance coverage.
Recent advances include long-acting injectable PrEP options, such as cabotegravir, which demonstrated superior efficacy compared with daily oral TDF-FTC in large randomized trials [91, 92]. These long-acting strategies may improve adherence and expand prevention options for young populations. Six-monthly lenacapavir and intravaginal dapivirine rings represent promising strategies to improve adherence and expand prevention options for young individuals at risk of HIV infection [93, 94]. Doxycycline post-exposure prophylaxis (Doxy-PEP) has demonstrated significant reductions in chlamydia and syphilis incidence when taken within 72 hours after exposure, although effectiveness against gonorrhea is variable due to resistance [95].
Another promising area involves vaccine development for bacterial and viral STIs, including vaccines targeting C. trachomatis, N. gonorrhoeae, T. pallidum, and HSV. Although several candidates are currently in early-phase clinical trials, scientific challenges related to pathogen immune evasion and antigenic variability remain significant obstacles [96]. Partner notification and treatment are essential components of STI control. However, implementation among adolescents and young adults remains challenging. In a study examining the STI care cascade in South Africa, although 100% of diagnosed individuals completed treatment, only 74% notified a sexual partner, and just 35% reported that partners received treatment [97]. Stigma, lack of knowledge about STIs, and concerns about relationship conflict represent common barriers to partner notification [97].
Screening and Testing Approaches
Regular screening remains a cornerstone of STI prevention among adolescents and young adults, particularly given the high prevalence of asymptomatic infections described earlier. Advances in diagnostic technologies and testing strategies have expanded access to screening.
Access to confidential, youth-friendly sexual health services is a critical determinant of whether adolescents seek STI prevention, testing, and treatment services. Confidentiality protections are particularly important for reproductive health services, including STI testing and treatment.
Adolescents frequently express concerns that STI diagnoses or testing may be disclosed to parents, which may discourage healthcare-seeking behavior [98].
Youth-centered service models, including school-based clinics, community outreach programs, and digital health interventions, have been shown to improve engagement with sexual health services among adolescents and young adults.
Self-collected specimens, including vaginal swabs and urine samples, have been shown to significantly increase testing uptake. A systematic review and meta-analysis found that offering self-collection methods approximately doubled STI testing uptake compared with facility-based testing, with a modest increase in case detection [99].
Similarly, HIV self-testing has emerged as a powerful strategy to expand testing access. Meta-analyses of randomized controlled trials demonstrate that providing self-testing kits results in approximately twice the testing frequency compared with standard testing services and leads to the identification of additional HIV-positive individuals without increasing sexual risk behaviors [100]. Community-based approaches further enhance case detection. Mobile testing services, home-based testing programs, and index partner testing have been particularly effective in reaching populations that may face barriers to facility-based care. Among testing strategies evaluated across several programs, mobile testing had the highest proportion of men, with approximately 50% of participants male, compared with lower participation rates in traditional clinic-based testing [101].
Behavioral and educational interventions
Comprehensive sexual education represents a fundamental component of STI prevention strategies among adolescents. Evidence indicates that school-based comprehensive sex education programs significantly improve knowledge, attitudes, and preventive behaviors related to sexual health [102]. In contrast, analyses of state-level data in the United States demonstrated that states emphasizing abstinence-only education experienced higher teenage pregnancy rates, suggesting that these programs may be ineffective or even counterproductive [103].
Behavioral interventions based on established psychological frameworks also show promise. Stepped-care behavioral models, incorporating elements such as communication skills training, assertiveness training, and problem-solving strategies, have demonstrated effectiveness in reducing STI risk behaviors and improving contraceptive use among adolescents [104].

Figure 2 presents an integrated framework for the prevention, screening, and control of STIs among adolescents and young adults.
CONCLUSIONS
STIs remain a major global public health challenge, disproportionately affecting adolescents and young adults aged 15–24 years. This age group accounts for a substantial proportion of new STI cases worldwide, reflecting the combined influence of biological vulnerability, behavioral risk factors, and structural determinants such as limited access to sexual health services, stigma, and social inequities. The epidemiology of STIs among young people is characterized by a high prevalence of asymptomatic infections, particularly for pathogens such as C. trachomatis, N. gonorrhoeae, and M. genitalium, which significantly limits the effectiveness of symptom-based diagnostic strategies. As highlighted in this review, adolescents and young adults are also affected by marked disparities related to gender, sexual orientation, socioeconomic status, and racial or ethnic background, with certain populations, including MSM, transgender youth, and young sex workers, experiencing a disproportionately high burden of infection. Although multiple effective prevention strategies are currently available, including vaccination, HIV PrEP prophylaxis, screening programs, behavioral interventions, and improved access to treatment, the implementation and uptake of these interventions remain uneven across settings and populations. Expanding access to youth-friendly and confidential sexual health services, increasing vaccine coverage, and promoting routine screening for asymptomatic infections are critical components of effective STI control strategies.
Strengthening sexual health education, reducing stigma, and developing innovative prevention approaches tailored to the needs of young populations will be essential to achieve sustainable improvements in sexual health outcomes worldwide.
Funding
None to declare.
Conflicts of interest
We declare no competing interests.
Authors contribution
LP and AC drafted and revised the manuscript. LP and GDA Figure and visualization.
REFERENCES
[1] Sexually transmitted infections (STIs). 2025. Available at: https://www.who.int/news-room/fact-sheets/detail/sexually-transmitted-infections-(stis). [Accessed 3 March 2026].
[2] Diana P, Esposito S. Epidemiology, risk factors, and prevention strategies of HIV, HPV, and other sexually transmitted infections among cisgender and transgender youth: a narrative review. Front Public Health 2024; 12: 1342532.
[3] Sexually Transmitted Infections among Young Americans. 2016. Available at: https://www.google.com/search?client=safari&rls=en&q=Sexually+Transmitted+Diseases%3A+Adolescents+and+young+adults.+Atlanta%3A+CDC%2C+https%3A%2F%2Fwww.cdc.gov%2Fstd%2Flife-stages-populations%2Fadolescents-+youngadults&ie=UTF-8&oe=UTF-8. [Accessed 3 March 2017].
[4] Pipitò L, Bono E, Tolomeo M, et al. Advances in the Management of MPOX Infection: Therapeutic and Vaccination Perspectives. Curr Treat Options Infect Dis 2025; 17: 12.
[5] 2024 global AIDS update. 2025. Available at: https://www.unaids.org/en/site-search#?cludoquery=global%20aids%20update%202025&cludopage=1&cludorefurl=https%3A%2F%2Fwww.unaids.org%2Fen&cludorefpt=UNAIDS&cludorefact=Global%20aids&cludorefaci=1&cludoinputtype=standard. [Accessed 3 March 2026].
[6] Matteelli A, Beltrame A, Carvalho AC, et al. Chlamydia trachomatis genital infection in migrant female sex workers in Italy. Int J STD AIDS. 2003; 14(9): 591-595.
[7] Workowski KA, Bachmann LH, Chan PA, et al. Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR Recomm Rep. 2021; 70(4): 1-187.
[8] Zanotta N, West N, Cason C, et al. New Trends in Sexually Transmitted Infections Among Adolescents and Young People: Epidemiology, Clinical and Diagnostic Management. Microorganisms 2025; 13(6): 1411.
[9] Rowley J, Vander Hoorn S, Korenromp E, et al. Chlamydia, gonorrhoea, trichomoniasis and syphilis: global prevalence and incidence estimates, 2016. Bull World Health Organ. 2019; 97(8): 548-562.
[10] Omosigho PO, Ajide TE, Izevbuwa OE, et al. Seroprevalence of Chlamydia trachomatis and associated risk factors among HIV positive women in North Central Nigeria. Infez Med. 2024; 32(1): 52-60.
[11] Ciccarese G, Pattaro M, Salvi I, et al. Detection of Chlamydia trachomatis, Neisseria gonorrhoeae and Ureaplasma urealyticum in symptomatic and asymptomatic subjects. Infez Med. 2025; 33(2): 247–248.
[12] Price MJ, Ades AE, Soldan K, et al. The natural history of Chlamydia trachomatis infection in women: a multi-parameter evidence synthesis. Health Technol Assess. 2016; 20(22): 1-250.
[13] Seraceni S, De Seta F, Colli C, et al. High prevalence of hpv multiple genotypes in women with persistent chlamydia trachomatis infection. Infect Agents Cancer 2014; 9: 30.
[14] Bragazzi NL, Bosch Castells V, Deng Q, et al. The Impact of Chlamydia trachomatis on Male Infertility: A Systematic Review and Meta-Analysis. Open Forum Infect Dis. 2025; 13(1): ofaf782.
[15] Lymphogranuloma venereum. Annual epidemiological report for 2023. 2025. Available at: https://www.ecdc.europa.eu/sites/default/files/documents/LGV_AER_2023_Report%20-%20final%20pdf.pdf. [Accessed 3 March 2026].
[16] Hughes Y, Chen MY, Fairley CK, et al. Universal lymphogranuloma venereum (LGV) testing of rectal chlamydia in men who have sex with men and detection of asymptomatic LGV. Sex Transm Infect. 2022; 98(8): 582-585.
[17] Gonorrhoea. Annual epidemiological report for 2022. 2024. Available at: https://www.ecdc.europa.eu/sites/default/files/documents/GONO_AER_2022_Report%20FINAL.pdf. [Accessed 3 March 2026].
[18] Aitolo GL, Adeyemi OS, Afolabi BL, et al. Neisseria gonorrhoeae Antimicrobial Resistance: Past to Present to Future. Curr Microbiol 2021; 78: 867-878.
[19] Cornelisse VJ, Chow EPF, Huffam S, et al. Increased Detection of Pharyngeal and Rectal Gonorrhea in Men Who Have Sex With Men After Transition From Culture To Nucleic Acid Amplification Testing. Sexual Trans Dis 2017; 44: 114–117.
[20] Syphilis. 2025. Available at: https://www.who.int/news-room/fact-sheets/detail/syphilis. [Accessed 26 March 2026].
[21] Syphilis. Annual Epidemiological Report for 2022. 2024. Available at: https://www.ecdc.europa.eu/sites/default/files/documents/SYPH_AER_2022_Report_0.pdf. [Accessed 3 March 2026].
[22] Mazzola CV, Bono E, Giacchino I, Calà C, Pipitò L, Cascio A. Malignant Syphilis in an Immunocompetent Patient: A Case Report and Review of the Literature. J Clin Med. 2025; 14(24): 8839.
[23] Pipitò L, Ganci I, Cicero A, et al. A Case of Syphilis With Ocular Involvement: Persistent Negative Serology in a Patient With Multiple Sclerosis. Open Forum Infect Dis. 2024; 11(10): ofae563.
[24] Pipitò L, Gaudiano R, Di Figlia F, et al. Interesting case of syphilis with atypical vegetative lesions. Sex Transm Infect. 2025; 101(4): 278-279.
[25] Pipitò L, Medaglia AA, Trizzino M, et al. A case of syphilis associated with immune reconstitution inflammatory syndrome and review of the literature. AIDS Res Ther. 2023; 20(1): 28.
[26] Pipitò L, Russotto I, Arena D, Calà C, Cascio A. Mucocutaneous relapse during late latent syphilis as initial presentation of HIV infection. IDCases. 2024; 37: e02062.
[27] Pipitò L, Piccione M, Trizzino M, Calà C, Cascio A. An Uncommon Case of Syphilis With Simultaneous, Different Lesions: Moth-Eaten Alopecia, Syphilitic Keratoderma, and Psoriasiform Syphilis. Cureus. 2023; 15(11): e49181.
[28] Pipitò L, Trizzino M, Orlando E, Calà C, Cascio A. Lepromatous nodular syphilis: A case from Italy. Travel Med Infect Dis. 2023; 53: 102564.
[29] Sifilide in Italia. 2022. Available at: https://www.epicentro.iss.it/sifilide/epidemiologia-italia. [Accessed 27 April 2026].
[30] Baumann L, Cina M, Egli-Gany D, et al. Prevalence of Mycoplasma genitalium in different population groups: systematic review andmeta-analysis. Sex Transm Infect. 2018; 94(4): 255-262.
[31] Lis R, Rowhani-Rahbar A, Manhart LE. Mycoplasma genitalium infection and female reproductive tract disease: a meta-analysis. Clin Infect Dis. 2015; 61(3): 418-426.
[32] Lam PPH, Nguyen NH, Nguyen TTT, Trinh NB, Luong BA. Mycoplasma genitalium prevalence, co-infection and macrolide resistance-associated mutations in Southern Vietnam. Infez Med. 2024; 32(2): 222-230.
[33] Fei LP, Zhao HH, Yang ZN, et al. HIV incidence and recreational drug use among men who have sex with men aged 18-24 years in Tianjin, China: a retrospective cohort study. BMC Infect Dis. 2024; 24(1): 1295.
[34] HIV/AIDS Surveillance in Europe 2024 – 2023 data. 2024. Available at: https://www.ecdc.europa.eu/en/publications-data/hiv-aids-surveillance-europe-2024-2023-data#:~:text=For%20the%20EU/EEA%20countries,reported%20than%20estimated%20new%20infections.&text=close%20the%20gap%20on%20undiagnosed,in%202023%20compared%20to%202022. [Accessed 4 March 2026].
[35] Artenie A, Stone J, Fraser H, et al. Incidence of HIV and hepatitis C virus among people who inject drugs, and associations with age and sex or gender: a global systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2023; 8(6): 533-552.
[36] Stoner MCD, Rucinski KB, Lyons C, Napierala S. Differentiating the incidence and burden of HIV by age among women who sell sex: a systematic review and meta-analysis. J Int AIDS Soc. 2022; 25(10): e26028.
[37] Kharsany AB, Karim QA. HIV Infection and AIDS in Sub-Saharan Africa: Current Status, Challenges and Opportunities. Open AIDS J. 2016; 10: 34-48.
[38] Baldeh M, Kizito S, Lakoh S, et al. Advanced HIV disease and associated factors among young people aged 15-24 years at a tertiary hospital in Sierra Leone: a cross-sectional study. BMC Infect Dis. 2024; 24(1): 611.
[39] Yu Q, Zhao H, Sun D, Liu Y, Yu Y. Prevalence and factors influencing HIV testing behavior in adolescents and young adults: a systematic review and meta-analysis. Prev Med Rep. 2025; 57: 103211.
[40] James C, Harfouche M, Welton NJ, et al. Herpes simplex virus: global infection prevalence and incidence estimates, 2016. Bull World Health Organ. 2020; 98(5): 315-329.
[41] Freeman EE, Weiss HA, Glynn JR, Cross PL, Whitworth JA, Hayes RJ. Herpes simplex virus 2 infection increases HIV acquisition in men and women: systematic review and meta-analysis of longitudinal studies. AIDS. 2006; 20(1): 73-83.
[42] Harfouche M, AlMukdad S, Alareeki A, et al. Estimated global and regional incidence and prevalence of herpes simplex virus infections and genital ulcer disease in 2020: mathematical modelling analyses. Sex Transm Infect. 2025; 101(4): 214-223.
[43] Giuliano AR, Felsher M, Waterboer T, et al. Oral Human Papillomavirus Prevalence and Genotyping Among a Healthy Adult Population in the US. JAMA Otolaryngol Head Neck Surg. 2023; 149(9): 783-795.
[44] Johnston C, Magaret A, Son H, et al. Viral Shedding 1 Year Following First Episode Genital HSV-1 Infection. JAMA. 2022; 328(17): 1730-1739.
[45] Pipitò L, Cascio A. Genital pustules, fever, lymphadenopathy in a heterosexual couple. Travel Med Infect Dis. 2022; 50: 102483.
[46] Lewis RM, Laprise JF, Gargano JW, et al. Estimated Prevalence and Incidence of Disease-Associated Human Papillomavirus Types Among 15- to 59-Year-Olds in the United States. Sex Transm Dis. 2021; 48(4): 273-277.
[47] Liu H, Duan S, Chu W, Yang R, Wei L, Zhang S. Age-specific prevalence of multiple human papillomavirus infections in a clinical cohort of men: a cross-sectional study in Shenzhen, China. Emerg Microbes Infect. 2026; 15(1): 2608402.
[48] Bruni L, Albero G, Rowley J, et al. Global and regional estimates of genital human papillomavirus prevalence among men: a systematic review and meta-analysis. Lancet Glob Health. 2023; 11(9): e1345-e1362.
[49] Prete RD, Ronga L, Addati G, et al. Prevalence, genotype distribution and temporal dynamics of human papillomavirus infection in a population in southern Italy. Infez Med. 2017; 25(3): 247-257.
[50] Human papillomavirus and cancer. 2024. Available at: https://www.who.int/news-room/fact-sheets/detail/human-papilloma-virus-and-cancer. [Accessed 4 March 2026].
[51] Williamson, Deborah A, and Marcus Y Chen. Emerging and Reemerging Sexually Transmitted Infections. N Engl J Med. 2020; 382(21): 2023-2032.
[52] Hofmeister MG, Xing J, Foster MA, et al. Hepatitis A Person-to-Person Outbreaks: Epidemiology, Morbidity Burden, and Factors Associated With Hospitalization-Multiple States, 2016-2019. J Infect Dis. 2021; 223(3): 426-434.
[53] Lanini S, Minosse C, Vairo F, et al. A large ongoing outbreak of hepatitis A predominantly affecting young males in Lazio, Italy; August 2016 - March 2017. PLoS One. 2017; 12(11): e0185428.
[54] Mpox. 2024. Available at: https://www.who.int/news-room/fact-sheets/detail/mpox. [Accessed 27 March 2026].
[55] Risk of Clade II Mpox Associated with Intimate and Nonintimate Close Contact Among Men Who Have Sex with Men and Transgender Adults — United States, August 2022–July 2023. 2024. Available at: https://www.cdc.gov/mmwr/volumes/73/wr/mm7340a2.htm?utm. [Accessed 27 March 2026].
[56] Beeson AM, Haston J, McCormick DW, et al. Mpox in Children and Adolescents: Epidemiology, Clinical Features, Diagnosis, and Management. Pediatrics. 2023; 151(2): e2022060179.
[57] Kissinger P. Trichomonas vaginalis: a review of epidemiologic, clinical and treatment issues. BMC Infect Dis. 2015; 15: 307.
[58] Coudray MS, Madhivanan P. Bacterial vaginosis-A brief synopsis of the literature. Eur J Obstet Gynecol Reprod Biol. 2020; 245: 143-148.
[59] Verstraelen H, Verhelst R, Vaneechoutte M, Temmerman M. The epidemiology of bacterial vaginosis in relation to sexual behaviour. BMC Infect Dis. 2010; 10: 81.
[60] Javed A, Parvaiz F, Manzoor S. Bacterial vaginosis: An insight into the prevalence, alternative treatments regimen and it’s associated resistance patterns. Microb Pathog. 2019; 127: 21-30.
[61] Bautista CT, Wurapa E, Sateren WB, Morris S, Hollingsworth B, Sanchez JL. Bacterial vaginosis: a synthesis of the literature on etiology, prevalence, risk factors, and relationship with chlamydia and gonorrhea infections. Mil Med Res. 2016; 3: 4.
[62] Vodstrcil LA, Plummer EL, Fairley CK, et al. Male-Partner Treatment to Prevent Recurrence of Bacterial Vaginosis. N Engl J Med. 2025; 392(10): 947-957.
[63] Alarming decline in adolescent condom use, increased risk of sexually transmitted infections and unintended pregnancies, reveals new WHO report. 2024. Available at: https://www.who.int/europe/news/item/29-08-2024-alarming-decline-in-adolescent-condom-use--increased-risk-of-sexually-transmitted-infections-and-unintended-pregnancies--reveals-new-who-report. [Accessed 5 March 2026].
[64] Haider MR, Kingori C, Brown MJ, Battle-Fisher M, Chertok IA. Illicit drug use and sexually transmitted infections among young adults in the US: evidence from a nationally representative survey. Int J STD AIDS. 2020; 31(13): 1238-1246.
[65] Rosas Cancio-Suárez M, Ron R, Díaz-Álvarez J, et al. Prevalence, characteristics, and associated risk factors of drug consumption and chemsex use among individuals attending an STI clinic (EpITs STUDY). Front Public Health. 2023; 11: 1285057.
[66] Satapathy P, Gaidhane AM, Vadia N, et al. Association of chemsex and risk of chlamydia, gonorrhoea, and syphilis infections: a systematic review and meta-analysis. Public Health. 2025; 249: 105971.
[67] Abreu C, Sá L, Santos P. Adolescents’ Knowledge and Misconceptions About Sexually Transmitted Infections: A Cross-Sectional Study in Middle School Students in Portugal. Healthcare (Basel). 2024; 12(22): 2283.
[68] Chang CC, Chen MH, Bai YM, Tsai SJ, Chen TJ, Liou YJ. Elevated risk of sexually transmitted infections among adolescents and young adults with borderline personality disorder: a retrospective longitudinal nationwide population-based study. Eur Child Adolesc Psychiatry. 2024; 33(12): 4185-4194.
[69] Chan CT, Ming K, Camp C, Saberi P. Sexual Behaviors, Substance Use, and Quality of Life Among Individuals Using PrEP in San Francisco During the COVID-19 Pandemic Shelter-In-Place Orders: A Cross-Sectional Survey. J Acquir Immune Defic Syndr. 2022; 89(4): e39-e42.
[70] Health Disparities in HIV, Viral Hepatitis, STDs, & Tuberculosis. Health Disparities in Black or African American People. Available at: https://www.cdc.gov/health-disparities-hiv-std-tb-hepatitis/populations/black-african-american.html [Accessed on 5 March 2026].
[71] Douglas CM, Ahrens K, Dombrowski JC, Rodean J, Coker TR. Racial and Ethnic Differences in Chlamydia and Gonorrhea Testing Locations Among Medicaid-Insured Youth. J Adolesc Health. 2024; 74(2): 381-384.
[72] Reisner SL, Jadwin-Cakmak L, Sava L, Liu S, Harper GW. Situated Vulnerabilities, Sexual Risk, and Sexually Transmitted Infections’ Diagnoses in a Sample of Transgender Youth in the United States. AIDS Patient Care STDS. 2019; 33(3): 120-130.
[73] Poteat VP, Calzo JP, Yoshikawa H, et al. Greater Engagement in Gender-Sexuality Alliances (GSAs) and GSA Characteristics Predict Youth Empowerment and Reduced Mental Health Concerns. Child Dev. 2020; 91(5): 1509-1528.
[74] Werner RN, Gaskins M, Nast A, Dressler C. Incidence of sexually transmitted infections in men who have sex with men and who are at substantial risk of HIV infection - A meta-analysis of data from trials and observational studies of HIV pre-exposure prophylaxis. PLoS One. 2018; 13(12): e0208107.
[75] Mondal NI, Hossain K, Islam R, Mian AB. Sexual behavior and sexually transmitted diseases in street-based female sex workers in Rajshahi City, Bangladesh. Braz J Infect Dis. 2008; 12(4): 287-292.
[76] Traeger MW, Cornelisse VJ, Asselin J, et al. Association of HIV Preexposure Prophylaxis With Incidence of Sexually Transmitted Infections Among Individuals at High Risk of HIV Infection. JAMA. 2019; 321(14): 1380-1390.
[77] Kaida A, Dietrich JJ, Laher F, et al. A high burden of asymptomatic genital tract infections undermines the syndromic management approach among adolescents and young adults in South Africa: implications for HIV prevention efforts. BMC Infect Dis. 2018; 18(1): 499.
[78] Kamolratanakul S, Pitisuttithum P. Human Papillomavirus Vaccine Efficacy and Effectiveness against Cancer. Vaccines (Basel). 2021; 9(12): 1413.
[79] Meites E, Szilagyi PG, Chesson HW, Unger ER, Romero JR, Markowitz LE. Human Papillomavirus Vaccination for Adults: Updated Recommendations of the Advisory Committee on Immunization Practices. MMWR Morb Mortal Wkly Rep. 2019; 68(32): 698-702.
[80] Guarducci G, Chiti M, Fattore DC, et al. Development of a network model to implement the HPV vaccination coverage. Ann Ig. 2024; 36(6): 636-643.
[81] Cartmell KB, Mzik CR, Sundstrom BL, et al. HPV Vaccination Communication Messages, Messengers, and Messaging Strategies. J Canc Educ 2019; 34: 1014–1023.
[82] Bruni L, Diaz M, Barrionuevo-Rosas L, et al. Global estimates of human papillomavirus vaccination coverage by region and income level: a pooled analysis. The Lancet Global Health 2016; 4: e453–e463.
[83] Hepatitis B Vaccine Administration. 2025. Available at: https://www.cdc.gov/hepatitis-b/hcp/vaccine-administration/index.html. [Accessed 5 March 2026].
[84] Nelson NP, Weng MK, Hofmeister MG, et al. Prevention of Hepatitis A Virus Infection in the United States: Recommendations of the Advisory Committee on Immunization Practices, 2020. MMWR Recomm Rep. 2020; 69(5): 1-38.
[85] Yin S, Barker L, Ly KN, et al.Susceptibility to Hepatitis A Virus Infection in the United States, 2007-2016. Clin Infect Dis. 2020; 71(10): e571-e579.
[86] Geng L, Whittles LK, Dickens BL, et al. Potential public health impacts of gonorrhea vaccination programmes under declining incidences: A modeling study. PLoS Med. 2025; 22(2): e1004521.
[87] Abara WE, Bernstein KT, Lewis FMT, et al. Effectiveness of a serogroup B outer membrane vesicle meningococcal vaccine against gonorrhoea: a retrospective observational study. Lancet Infect Dis. 2022; 22(7): 1021-1029.
[88] Grant RM, Lama JR, Anderson PL, et al. Preexposure chemoprophylaxis for HIV prevention in men who have sex with men. N Engl J Med. 2010; 363(27): 2587-2599.
[89] Molina JM, Charreau I, Chidiac C, et al. Post-exposure prophylaxis with doxycycline to prevent sexually transmitted infections in men who have sex with men: an open-label randomised substudy of the ANRS IPERGAY trial. Lancet Infect Dis. 2018; 18(3): 308-317.
[90] Adeagbo O. Barriers and facilitators to pre-exposure prophylaxis uptake among Black/African American men who have sex with other men in Iowa: COM-B model analysis. Ther Adv Infect Dis. 2024; 11: 20499361241267151.
[91] Landovitz RJ, Hanscom BS, Clement ME, et al. Efficacy and safety of long-acting cabotegravir compared with daily oral tenofovir disoproxil fumarate plus emtricitabine to prevent HIV infection in cisgender men and transgender women who have sex with men 1 year after study unblinding: a secondary analysis of the phase 2b and 3 HPTN 083 randomised controlled trial. Lancet HIV. 2023; 10(12): e767-e778.
[92] Delany-Moretlwe S, Hughes JP, Bock P, et al. Cabotegravir for the prevention of HIV-1 in women: results from HPTN 084, a phase 3, randomised clinical trial. Lancet. 2022; 399(10337): 1779-1789.
[93] Sah S, Iqbal U, Mishra T, Ullah N, Yadav T. Twice-Yearly Injectable Pre-Exposure Prophylaxis With Lenacapavir: Redefining Adherence and Access in the Global Fight Against HIV. J Int Assoc Provid AIDS Care. 2025; 24: 23259582251390622.
[94] Noguchi LM, Owor M, Mgodi NM, et al. Safety and drug quantification of the dapivirine vaginal ring and oral pre-exposure prophylaxis in breastfeeding mother-infant pairs (MTN-043): a phase 3B, open-label, randomised trial. Lancet HIV. 2025; 12(3): e180-e190.
[95] Sokoll PR, Migliavaca CB, Döring S, Traub U, Stark K, Sardeli AV. Efficacy of postexposure prophylaxis with doxycycline (Doxy-PEP) in reducing sexually transmitted infections: a systematic review and meta-analysis. Sex Transm Infect. 2025; 101(1): 59-67.
[96] Gökengin D, Noori T, Alemany A, et al. Prevention strategies for sexually transmitted infections, HIV, and viral hepatitis in Europe. Lancet Reg Health Eur. 2023; 34: 100738.
[97] Chitneni P, Beksinska M, Dietrich JJ, et al. Partner notification and treatment outcomes among South African adolescents and young adults diagnosed with a sexually transmitted infection via laboratory-based screening. Int J STD AIDS. 2020; 31(7): 627-636.
[98] Maslyanskaya S, Alderman EM. Confidentiality and Consent in the Care of the Adolescent Patient. Pediatr Rev. 2019; 40(10): 508-516.
[99] Ogale Y, Yeh PT, Kennedy CE, Toskin I, Narasimhan M. Self-collection of samples as an additional approach to deliver testing services for sexually transmitted infections: a systematic review and meta-analysis. BMJ Glob Health. 2019; 4(2): e001349.
[100] Johnson CC, Kennedy C, Fonner V, et al. Examining the effects of HIV self-testing compared to standard HIV testing services: a systematic review and meta-analysis. J Int AIDS Soc. 2017; 20(1): 21594.
[101] Sharma M, Ying R, Tarr G, Barnabas R. Systematic review and meta-analysis of community and facility-based HIV testing to address linkage to care gaps in sub-Saharan Africa. Nature. 2015; 528(7580): S77-S85.
[102] Fonner VA, Armstrong KS, Kennedy CE, O’Reilly KR, Sweat MD. School based sex education and HIV prevention in low- and middle-income countries: a systematic review and meta-analysis. PLoS One. 2014; 9(3): e89692.
[103] Stanger-Hall KF, Hall DW. Abstinence-only education and teen pregnancy rates: why we need comprehensive sex education in the U.S. PLoS One. 2011; 6(10): e24658.
[104] Desrosiers A, Betancourt T, Kergoat Y, Servilli C, Say L, Kobeissi L. A systematic review of sexual and reproductive health interventions for young people in humanitarian and lower-and-middle-income country settings. BMC Public Health. 2020; 20(1): 666.