Le Infezioni in Medicina, n. 2, 164-176, 2026
doi: 10.53854/liim-3402-6
REVIEW
Nipah virus infection: what clinicians need to know
Nitin Gupta1, Shreya Das Adhikari2, Mukund Gupta3, Sonali Singh4, Tirlangi Praveen Kumar1, Alfonso J. Rodriguez-Morales5,6, Carl Boodman7
1 Department of Infectious Disease, Kasturba Medical College, Manipal Academy of Higher Education, Manipal, India;
2 Department of Anaesthesiology, Kasturba Medical College, Manipal Academy of Higher Education, Manipal, India;
3 All India Institute of Medical Sciences, Jodhpur, India;
4 Division of Neurology, Department of Paediatrics, Hospital for Sick Children, University of Toronto, Toronto, Ontario, Canada.
5 Faculty of Health Sciences, Universidad Científica del Sur, Lima, Peru;
6 Grupo de Investigación Biomedicina, Faculty of Medicine, Fundación Universitaria Autónoma de las Américas-Institución Universitaria Visión de las Américas, Pereira, Colombia;
7 Department of Clinical Sciences, Institute of Tropical Medicine, Antwerp, Belgium.
Article received 20 March 2026 and accepted 11 May 2026
Corresponding author
Nitin Gupta
E-mail: nitin.gupta@manipal.edu
SUMMARY
Nipah virus infection is an uncommon but highly lethal zoonotic illness that primarily presents with acute encephalitis and respiratory disease in humans. After its initial identification during the Malaysia–Singapore outbreak of 1998–1999, human outbreaks have since been reported in Bangladesh and India. Despite the relatively small number of reported cases, the Nipah virus remains a major clinical and public health concern because of its high mortality, capacity for person-to-person transmission, lack of approved antiviral treatment, and potential for amplification within healthcare settings. For clinicians, the major challenge lies in early recognition of a disease that initially presents with nonspecific febrile symptoms but may rapidly progress to severe encephalitis, acute respiratory distress syndrome, or both. Human-to-human transmission has been well documented in South Asian outbreaks, particularly in household and healthcare settings, underscoring the importance of prompt isolation and infection prevention measures. Laboratory confirmation relies primarily on reverse transcription polymerase chain reaction, with serology providing supportive evidence later in the course of illness. Management remains largely supportive, with intensive care often required in severe cases. This review provides a practical clinician-oriented overview of Nipah virus infection, focusing on epidemiology relevant to frontline practice, clinical presentation, transmission, diagnostic approach, infection control, treatment, prognosis, and outbreak response.
Keywords: Nipah virus, encephalitis, acute respiratory distress syndrome, outbreak, diagnosis, infection prevention, zoonosis.
INTRODUCTION
Nipah virus infection is a rare but often fatal zoonotic disease that causes acute encephalitis and respiratory illness in humans [1, 2]. The virus belongs to the genus Henipavirus, which also includes Hendra virus, within the family Paramyxoviridae, and is maintained in nature by fruit bats of the genus Pteropus [3]. Since its first recognition during an outbreak in Malaysia and Singapore in 1998–1999, the Nipah virus has caused sporadic outbreaks in South and Southeast Asia, with most human infections subsequently reported from Bangladesh and India [3-6]. Although the overall number of cases remains relatively small, the infection has attracted sustained attention because of its high case fatality rate, potential for limited human-to-human transmission, and the absence of licensed vaccines or specific antiviral therapies [3, 7]. Several outbreaks have also involved transmission to healthcare workers and household contacts, underscoring the clinical and public health implications of delayed recognition [7].
Given these characteristics, infectious disease clinicians and travel medicine practitioners need to be familiar with the basic clinical and epidemiological features of Nipah virus infection. Patients may initially present with a nonspecific febrile illness that can progress rapidly to encephalitis or severe respiratory disease, and the diagnosis may not be apparent immediately in settings where other causes of encephalitis are more common. This review focuses on the key clinical aspects of Nipah virus infection that are most relevant to practising clinicians, including epidemiology, clinical presentation, transmission, diagnostic approaches, infection prevention, and current management strategies.
EPIDEMIOLOGY RELEVANT TO CLINICAL PRACTICE
Human Nipah virus infection was first identified during a large outbreak among pig farmers in Malaysia and abattoir workers in Singapore in 1998–1999 (Figure 1) [3, 4, 8, 9]. In the Malaysian outbreak, pigs acted as amplifying hosts, and transmission to humans occurred primarily through close contact with infected animals [4]. In the 2014 outbreak in the Philippines, horses were identified as the likely amplifying host. In contrast, outbreaks reported since 2001 in Bangladesh and India have usually resulted from bat-to-human spillover, sometimes followed by limited but clinically important human-to-human transmission [6, 10, 11]. Bangladesh has reported recurrent outbreaks, while India has documented outbreaks in West Bengal and repeated events in Kerala [5, 6].
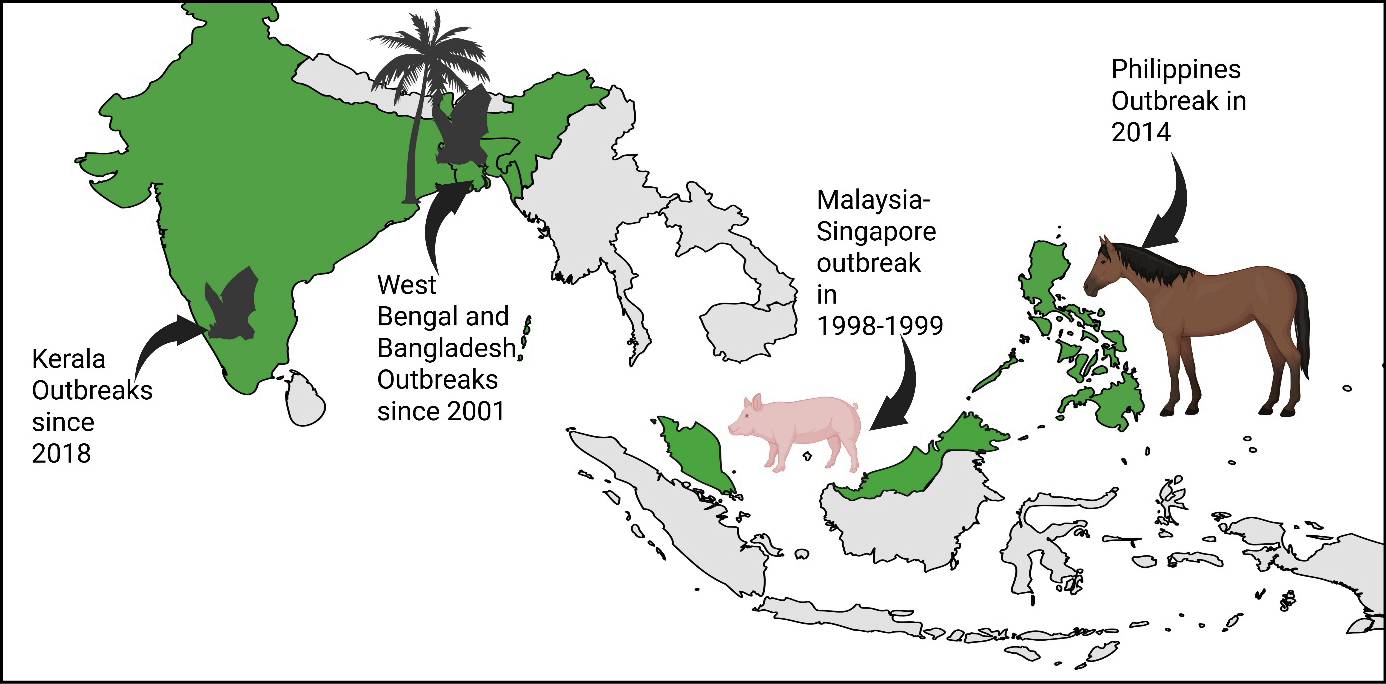
Figure 1 - Geographic distribution of major recognised Nipah virus outbreaks.
Note: The first large outbreak occurred in Malaysia, spreading to Singapore from 1998 to 1999, where pigs served as important amplifying hosts in transmission to humans. This was followed by recurrent outbreaks in Bangladesh since 2001, where fruit bats of the genus Pteropus are the natural reservoir, and spillover to humans has been linked to bat contamination of raw date palm sap. More recent outbreaks have been reported from Kerala, India, since 2018. In the Philippines, a separate outbreak was recognised in 2014 and was associated with horses. Green shading indicates locations of major recognised human outbreaks. At the same time, the pig, bat, palm tree, and horse icons denote the principal reservoir, spillover source, or amplifying host associated with each epidemiological setting. Image created using BioRender.
The pattern of transmission has differed across major outbreaks. In the Malaysia–Singapore outbreak, transmission was predominantly driven by exposure to infected pigs, and sustained human-to-human transmission was not a dominant feature [4]. In contrast, outbreaks in Bangladesh and India have more often involved bat-to-human spillover followed by person-to-person transmission, particularly in households and healthcare settings [6, 10, 11]. Several factors may contribute to this difference, including viral lineage, greater frequency of respiratory involvement, intensity of caregiving exposure, delayed recognition, and gaps in infection prevention. Although viral adaptations may influence transmissibility, current evidence does not support a simple explanation based solely on viral genetics. Transmission appears to depend on interactions among viral factors, clinical phenotype, exposure intensity, and healthcare practices.
Several epidemiological features are directly relevant to clinical suspicion. Most outbreaks in Bangladesh and West Bengal, India, have occurred during cooler months, often in association with ecological or behavioural exposures that facilitate spillover from bats [12, 13]. These include harvesting and consumption of bat-contaminated raw date palm sap, particularly in Bangladesh [12]. Outbreaks in Kerala, India, however, have predominantly occurred in April-May, likely coinciding with the fruiting season [14].
Although Pteropus bats are widely distributed across South and Southeast Asia, human infection remains uncommon, suggesting that spillover requires a combination of ecological, behavioural, and healthcare-related factors [15]. Thus, Nipah virus should be considered an uncommon disease with serious consequences rather than a common cause of febrile illness, but one in which delayed recognition may have serious implications for patient outcomes and outbreak control.
Human-to-human transmission has been documented in multiple Nipah virus outbreaks, particularly in Bangladesh and India since 2001. It represents a major mechanism by which outbreaks expand after the initial zoonotic spillover event [6, 10, 16, 17] (Table 1). Secondary infections most commonly occur among household caregivers or healthcare workers who have close contact with infected patients during illness. Transmission is believed to occur primarily through direct exposure to respiratory secretions, saliva, or other body fluids, particularly during advanced disease when patients develop severe neurological or respiratory manifestations [7]. Importantly, sustained airborne transmission has not been demonstrated, and most transmission chains remain limited once appropriate infection prevention and control measures are implemented [7].
Table 1 - Human-to-human transmission reported in selected Nipah virus outbreaks.
|
Author, Year |
Location/outbreak |
Total cases |
Human-to-human transmission and key setting |
|
Chadha |
Siliguri, India, |
66 |
50 cases, 75.8%, had documented exposure to healthcare facilities, suggesting predominantly nosocomial transmission involving healthcare workers, caregivers, and patients |
|
Hossain |
Bangladesh outbreaks, 2001 to 2004 |
92 |
32 cases were linked to contact with infected individuals, occurring mainly among household caregivers and healthcare contacts |
|
Pallivalappil |
Kerala, India, |
23 |
22 secondary cases were linked to contact with the index case, with transmission occurring predominantly in healthcare settings |
|
Anoop Kumar |
Kerala, India, |
6 |
5 secondary cases occurred among household and healthcare contacts of the primary case |
Note: Data are presented as reported in the original outbreak investigations. Percentages are calculated using the total number of reported cases in each outbreak. Human-to-human transmission includes probable or documented transmission in healthcare, household, or caregiver settings, as defined by the respective authors.
Evidence from outbreak investigations highlights the importance of healthcare settings in amplifying transmission. During the encephalitis outbreak in Siliguri, India, 50 of 66 patients, 75.8%, had documented exposure to healthcare facilities, suggesting extensive nosocomial transmission involving healthcare workers, caregivers, and other hospital contacts [6]. Similarly, investigations of outbreaks in Bangladesh between 2001 and 2004 identified 32 of 92 cases linked to contact with infected individuals, demonstrating the role of close household caregiving and healthcare exposure in disease propagation [10]. More recent outbreaks in southern India illustrate similar patterns. In the 2018 outbreak in Kerala, 22 of 23 cases represented secondary infections linked to the index case, with most transmission events occurring in healthcare settings before strict infection control measures were implemented [16]. Likewise, during the 2023 outbreak in Kerala, five of six confirmed cases occurred among household or healthcare contacts of the primary case [17].
Broader epidemiological analyses reinforce the importance of person-to-person spread in sustaining outbreaks once spillover has occurred. Over 14 years of outbreak investigations in Bangladesh, person-to-person transmission accounted for 82 of 248 cases, with a mean reproduction number of 0.33, and the risk of onward spread was greatest in older patients with respiratory symptoms and among contacts with prolonged exposure or contact with body fluids [18]. A recent systematic review of transmission dynamics in Bangladesh and India estimated that 133 of 189 cases (70%) were linked to exposure to another Nipah virus case, with 46% occurring in healthcare settings and 54% in community settings [7]. Transmission events were highly heterogeneous, with 71% of secondary cases arising from only six primary cases, suggesting superspreading-like events [7]. Despite this heterogeneity, transmission chains were generally short, with a mean of 0.83 secondary cases per infected individual and an average chain length of approximately 1.43 generations [7]. Exposure histories from the same review showed that transmission most often occurred through direct physical contact, exposure to body fluids, or prolonged exposure in the same room as an infected patient. At the same time, a small number of cases were linked to contact after death [7]. A meta-analysis further demonstrated that contact with a Nipah virus case was strongly associated with infection, with an odds ratio of 6.99 (95% CI 4.37-11.18) [7].
These findings indicate that most infected individuals do not transmit the virus widely, but a small number of primary cases may generate a disproportionate number of secondary infections. Such superspreading-like events are most likely when patients have severe respiratory or neurological disease, require close physical care, have exposure to body fluids, or are managed in crowded healthcare settings before Nipah virus infection is suspected. Overall, Nipah virus transmission between humans typically occurs through prolonged close contact in healthcare facilities or households. This reinforces the importance of early syndromic recognition, rapid isolation, appropriate PPE, safe respiratory care, monitoring of healthcare and household contacts, and strict infection prevention practices to prevent outbreak amplification.
CLINICAL PRESENTATION
The incubation period of Nipah virus infection typically ranges from 4 to 14 days. Observational data from Malaysian and Indian outbreaks suggest a usual interval of around 9-10 days between exposure and symptom onset [4, 9, 16]. In the 2018 Kerala outbreak, the median incubation period was 9.5 days, with a range of 4-14 days [16].
The illness usually begins with nonspecific symptoms that resemble many other acute viral infections. Fever is almost universal [3]. Headache, myalgia, fatigue, nausea, vomiting, sore throat, and dizziness may occur during the early phase, often making the disease clinically indistinguishable from other tropical febrile illnesses. In the Bangladesh clinical series, fever was universal, and headache, vomiting, and severe weakness were commonly reported [10]. In Kerala 2018, fever was present in all documented patients, with altered sensorium and shortness of breath also commonly observed [16].
Neurological involvement is the dominant clinical hallmark and most commonly presents as acute encephalitis. Patients may develop confusion, altered consciousness, seizures, focal deficits, myoclonus, and rapidly progressive neurological decline [3]. Early Malaysian outbreak studies described segmental myoclonus, reduced deep tendon reflexes, and autonomic features such as tachycardia and hypertension, suggesting brainstem and autonomic involvement [4, 9]. In Bangladesh, altered mental status and unconsciousness were frequent features [10]. In Kerala 2018, tachycardia, hypertension, and segmental myoclonus were also reported [16]. Death among fatal cases may occur within a median of six days from symptom onset, underscoring the rapid progression of severe disease [10].
Respiratory manifestations are also common and are particularly prominent in Bangladesh-lineage and Indian outbreaks. Patients may present with cough, dyspnoea, tachypnoea, hypoxaemia, pneumonia, or acute respiratory distress syndrome. In the Bangladesh series, respiratory symptoms, including cough and respiratory difficulty, were commonly reported [10]. The 2023 Kerala outbreak again demonstrated the mixed neuro-respiratory nature of the disease, with cases presenting with acute respiratory distress syndrome and encephalitis syndrome [17]. These findings are consistent with pooled data from a recent systematic review, which showed that Nipah virus disease frequently presents as a combined neurological and respiratory syndrome [3].
Neuroimaging abnormalities are not specific but may support the diagnosis and help define disease severity. Magnetic resonance imaging studies from Malaysian and Singaporean cohorts have shown multifocal small lesions, often within the white matter, consistent with microinfarction or inflammatory injury [19]. Delayed or relapsing encephalitis has also been reported among survivors, sometimes months or years after apparent recovery, suggesting persistent or recrudescent central nervous system involvement [20]. Long-term sequelae are increasingly recognised and may include gait disturbance, chronic fatigue, cognitive impairment, sleep disturbance, personality change, and seizure disorders. Survivor cohorts from Bangladesh demonstrate that persistent neurological and functional impairment is common in those who survive acute infection [21].
All characteristics of the key clinical studies of Nipah virus infection in humans are summarised in Table 2.
Table 2 - Key clinical studies of Nipah virus infection in humans.
|
Author, Year |
Study design, setting, period, |
Clinical profile |
Mortality |
|
Goh et al., |
Prospective clinical series, Malaysia, 1999 outbreak |
Fever, headache, and acute encephalitis were common, with reduced consciousness, seizures, segmental myoclonus, and brainstem dysfunction |
32% |
|
Chong et al., 2002 (n=103) |
Retrospective clinical cohort, Seremban Hospital, Malaysia, December 1998 to April 1999 |
Febrile encephalitic illness with headache, myalgia, vomiting, drowsiness, confusion, myoclonus, and dysautonomia, ventilation required in 61% |
41% |
|
Lim et al., |
Prospective MRI follow-up study, Singapore, follow-up of the 1999 outbreak |
Multifocal white matter MRI lesions with persistent neurological deficits and delayed complications in some survivors |
Not applicable |
|
Ng et al., |
Prospective follow-up study, Singapore, long-term follow-up |
Persistent neuropsychiatric sequelae, including depression, personality change, fatigue, |
Not applicable |
|
Chadha et al., 2006 (n=66) |
Outbreak investigation, Siliguri, India, January to February 2001 |
Fever, altered sensorium, encephalitis, seizures, and respiratory symptoms were common |
Approximately 74% |
|
Hossain et al., 2008 (n=92) |
Multicentre outbreak investigation, Bangladesh, outbreaks during 2001 to 2004 |
Fever was universal, with altered mental status, headache, respiratory distress, cough, and seizures common |
73% |
|
Pallivalappil |
Clinico-epidemiological outbreak study, Kerala, India, |
Fever, altered sensorium, tachycardia, hypertension, segmental myoclonus, |
91.3% |
|
Anoop Kumar |
Clinico-epidemiological outbreak investigation, Kozhikode, Kerala, India, 2023 outbreak |
Mixed presentation of acute respiratory |
33.3% |
|
Aquib et al., |
Cross-sectional survivor cohort study, Bangladesh, long-term follow-up of outbreak survivors |
Persistent sequelae, including gait disturbance, sleep disturbance, chronic fatigue, myoclonus, and cognitive impairment, were common |
Not applicable |
Note: Mortality is presented as reported in the original studies and may refer to case fatality within the study cohort rather than the entire outbreak. “Not applicable” indicates follow-up studies of survivors in which acute mortality was not the primary outcome. The clinical features shown are the predominant manifestations highlighted by each study and do not constitute an exhaustive list.
DIAGNOSTIC APPROACH
For frontline clinicians, Nipah virus infection should be approached as a syndromic condition rather than as an isolated rare diagnosis. Suspicion should be raised when any of the following patterns occur in an endemic or outbreak-prone region: sudden clustering of acute encephalitis cases in a community, severe respiratory illness with rapid deterioration, a mixed encephalitic and respiratory syndrome, illness among household caregivers of a similar patient, or disease among healthcare workers who cared for a patient with acute encephalitis or severe pneumonia. A single sporadic case may be difficult to recognise early because initial symptoms are non-specific. However, the combination of rapid neurological deterioration, respiratory involvement, high mortality, and epidemiological linkage should trigger immediate isolation, public health notification, and diagnostic testing for Nipah virus. This syndromic approach is especially important in emergency departments and primary care settings, where the first opportunity for containment may occur before laboratory confirmation is available.
The differential diagnosis should be considered after identifying the clinical syndrome and epidemiological context. Nipah virus infection overlaps with several common causes of acute encephalitis and severe respiratory illness in South and Southeast Asia. No single clinical feature reliably distinguishes Nipah virus infection from these conditions. Instead, diagnostic suspicion is strengthened by the combination of encephalitis, respiratory involvement, rapid progression, clustering, high case fatality, and linkage to household, healthcare, or zoonotic exposure, including bats or bat-contaminated date palm sap. In South and Southeast Asia, important neurological differentials include Japanese encephalitis, herpes simplex encephalitis, bacterial meningitis, cerebral malaria, scrub typhus with central nervous system involvement, dengue encephalopathy, and leptospirosis (Table 3) [22, 23]. Respiratory presentations may resemble severe influenza, SARS-CoV-2 infection, or other viral pneumonias [24].
Table 3 - Differential diagnoses of Nipah virus infection and distinguishing clinical features.
|
Syndrome |
Important differential diagnosis |
Overlap with Nipah virus infection |
Clues that may help distinguish from the Nipah virus |
|
Acute encephalitis syndrome |
Japanese encephalitis |
Fever, altered sensorium, seizures, encephalitis |
Mosquito exposure, rural or rice-field setting, seasonal transmission, predominantly neurological disease without prominent respiratory involvement |
|
Herpes simplex encephalitis |
Fever, seizures, altered behaviour, focal neurological deficits |
Usually sporadic, no outbreak clustering, temporal |
|
|
Bacterial meningitis |
Fever, altered mental status, seizures, and meningeal signs |
Prominent meningism, neutrophilic CSF pattern, bacterial pathogen identified on Gram stain, culture, or molecular testing, less commonly associated with respiratory failure or outbreak clustering |
|
|
Cerebral malaria |
Fever, coma, seizures, encephalopathy |
Travel or residence in a malaria-endemic area, parasitaemia on smear or rapid diagnostic test, anaemia, thrombocytopenia, or haemolysis |
|
|
Scrub typhus with CNS involvement |
Fever, encephalopathy, meningoencephalitis |
Eschar, thrombocytopenia, transaminitis, relevant |
|
|
Dengue encephalopathy |
Fever, altered sensorium, seizures in severe cases |
Rash, myalgia, thrombocytopenia, plasma leakage, bleeding manifestations, and epidemiological context |
|
|
Leptospirosis |
Fever, headache, encephalopathy, renal or hepatic dysfunction |
Conjunctival suffusion, jaundice, renal dysfunction, myalgia, exposure to contaminated water or animals |
|
|
Severe respiratory illness or ARDS |
Severe influenza |
Fever, cough, dyspnoea, viral pneumonia, ARDS |
Seasonal circulation, respiratory-predominant disease, |
|
SARS-CoV-2 infection |
Fever, cough, hypoxaemia, viral pneumonia, occasional encephalopathy |
Broader community transmission, respiratory predominance, compatible exposure history, confirmation by SARS-CoV-2 testing |
|
|
Other viral pneumonias |
Fever, cough, dyspnoea, hypoxaemia |
Usually, respiratory-predominant illness without |
Abbreviations: ARDS, acute respiratory distress syndrome; CNS, central nervous system; CSF, cerebrospinal fluid.
Note: The table highlights selected differential diagnoses of Nipah virus infection in South and Southeast Asia, organised by presenting syndrome. Distinguishing features are intended as practical clinical clues and should be interpreted in the context of epidemiological factors, laboratory findings, and local patterns of disease transmission.
Once Nipah virus infection is suspected, diagnostic testing should proceed in parallel with isolation and public health notification. Testing should not delay infection prevention measures. The preferred diagnostic test during acute illness is RT-PCR, but the optimal specimen depends on the clinical syndrome, timing of illness, and local laboratory capacity. In early acute illness or respiratory-predominant disease, throat, nasopharyngeal, or oropharyngeal swabs and blood are useful for RT-PCR testing. At the same time, CSF should be collected in patients with encephalitic presentations (Table 4) [17, 25]. However, CSF may be negative early in the disease, and a negative CSF RT-PCR should not exclude Nipah virus infection when the epidemiological and clinical context is suggestive.
Table 4 - Diagnostic approach to suspected Nipah virus infection.
|
Clinical situation |
Preferred specimen(s) |
Most useful test |
Key caveat |
|
Early acute illness |
Throat, nasopharyngeal, |
RT-PCR |
Best test for confirming acute infection, |
|
Encephalitic presentation |
CSF, respiratory swab, blood |
RT-PCR; |
CSF may be negative early, so respiratory |
|
Respiratory-predominant illness |
Throat, nasopharyngeal, |
RT-PCR |
Respiratory samples are particularly important when cough, dyspnoea, pneumonia, or ARDS |
|
Mixed neuro-respiratory syndrome |
Respiratory swab, blood, CSF if encephalitis |
RT-PCR; later serology |
Testing more than one specimen type may |
|
Later presentation or retrospective diagnosis |
Serum |
IgM and IgG serology |
Serology may be negative early and should |
|
Decentralised |
Validated specimen, depending on the available platform |
Point-of-care molecular assay, where available |
Availability and validation remain limited; confirmatory testing may still be needed |
|
Sample collection and transport |
All suspected high-risk specimens |
Not applicable |
Use trained staff, appropriate PPE, leak-proof containers, triple packaging, cold-chain transport, and prior communication with the receiving laboratory |
|
Negative test despite high suspicion |
Repeat or additional specimens guided by |
Repeat RT-PCR and/or serology |
A single negative result should not exclude |
Abbreviations: ARDS, acute respiratory distress syndrome; CSF, cerebrospinal fluid; IgG, immunoglobulin G; IgM, immunoglobulin M; PPE, personal protective equipment; RT-PCR, reverse transcription polymerase chain reaction.
Table note: Diagnostic testing should proceed in parallel with isolation, infection prevention measures, and public health notification. Testing should not delay clinical stabilisation or outbreak control.
Serological assays detecting Nipah-specific IgM and IgG can support diagnosis later in the course of illness and are useful for retrospective diagnosis and surveillance. Still, they may be negative during the early acute phase. False-negative results may occur because of low viral load, very early or late sampling, inappropriate specimen selection, inadequate sample volume, poor storage conditions, RNA degradation, or delays in transport to the reference laboratory. False-positive results are uncommon but may occur because of laboratory contamination, non-specific serological reactivity, or testing in low-pretest-probability settings. Therefore, diagnostic results should always be interpreted in relation to the clinical syndrome, exposure history, outbreak context, and local public health guidance.
The current diagnostic landscape remains limited, particularly for field-appropriate point-of-care testing, and most available assays still require specialised laboratory infrastructure [25]. Because the Nipah virus is a high-consequence pathogen, specimen collection and transport require careful coordination with designated public health and reference laboratories [26]. Samples should be collected by trained personnel using appropriate PPE, placed in leak-proof containers with triple packaging, clearly labelled as suspected high-risk infectious material, and transported under recommended cold-chain conditions. Unnecessary handling, centrifugation, aliquoting, or testing in non-designated laboratories should be avoided. In outbreak settings, clinicians should notify laboratory and public health teams before sample dispatch so that biosafety, documentation, transport, and testing pathways are activated promptly.
INFECTION PREVENTION AND CONTROL
Strict infection prevention and control measures are essential when managing patients with suspected or confirmed Nipah virus infection, as healthcare-associated transmission has been repeatedly documented [7]. Infection prevention measures should begin as soon as Nipah virus infection is suspected, without waiting for laboratory confirmation. Suspected cases should be isolated promptly, ideally in a single room with restricted access. Healthcare workers should use gloves, gowns, medical masks, and eye protection, with N95 or equivalent respirators during aerosol-generating procedures. Hand hygiene, careful donning and doffing of protective equipment, safe specimen handling, and frequent disinfection of high-touch surfaces are critical [7].
Nosocomial transmission has often coincided with deficiencies in basic infection prevention practices. Outbreak reports from Siliguri and Kerala described overcrowded wards, poor ventilation, inconsistent use of personal protective equipment, inadequate hand hygiene, and surface contamination as factors contributing to amplification [6, 7, 16]. Close contacts, including household members and healthcare workers, should be identified early and monitored for symptoms for at least 21 days.
In low- and middle-income settings, infection prevention should be based on early recognition, rapid isolation, and consistent implementation of simple high-impact measures. Healthcare facilities in outbreak-prone areas should have a predefined triage pathway for patients presenting with acute encephalitis, severe respiratory illness, or a compatible neuro-respiratory syndrome with clustering or contact history. Suspected cases should be immediately separated from crowded waiting areas and placed in a single room or a well-ventilated designated area with restricted access. If negative-pressure rooms are unavailable, a physically separated room with good natural ventilation and minimal staff movement is preferable to management in an open ward.
A small, trained team should be assigned to care for suspected or confirmed cases, and non-essential visitors should be restricted. Standard, contact, and droplet precautions should be applied for all suspected cases, with airborne precautions during aerosol-generating procedures such as intubation, suctioning, bronchoscopy, non-invasive ventilation, or cardiopulmonary resuscitation. Facilities should establish supervised donning and doffing areas, ensure hand hygiene at the point of care, disinfect high-touch surfaces frequently, and use safe protocols for waste management, linen handling, sharps disposal, and body handling. Contact tracing should begin as soon as a case is suspected, with early involvement of public health teams for exposure assessment, risk stratification, monitoring, and outbreak containment.
CLINICAL MANAGEMENT AND OUTCOMES
Management of suspected Nipah virus infection requires simultaneous attention to clinical stabilisation, infection prevention, and outbreak containment. Patients may deteriorate rapidly because of encephalitis, respiratory failure, autonomic dysfunction, or multiorgan involvement. Therefore, suspected cases should be managed in a setting capable of isolation, close monitoring, supportive care, and early escalation to intensive care where feasible. At the same time, contact tracing, healthcare worker protection, and public health coordination should begin immediately. Key components of management include airway protection, respiratory support, seizure control, management of raised intracranial pressure, haemodynamic stabilisation, and close monitoring for organ dysfunction (Table 5) [27]. Mechanical ventilation may be required in patients with severe pneumonia, acute respiratory distress syndrome, or reduced consciousness [27].
Table 5 - Practical management of patients with suspected or confirmed Nipah virus infection.
|
Clinical or public health issue |
Practical management priorities |
Key points |
|
Place of management |
Admit to a centre or designated area capable |
Severe cases may deteriorate rapidly because of encephalitis, respiratory failure, autonomic dysfunction, or multiorgan involvement |
|
Immediate isolation |
Place suspected cases in a single room or |
Isolation should begin when Nipah virus infection is suspected and should not wait |
|
PPE |
Gloves, gown, medical mask, and eye protection |
PPE should be used from the time Nipah virus infection is suspected |
|
Encephalitis |
Neurological monitoring, seizure control, airway protection, and management of raised intracranial pressure, where clinically indicated |
Rapid neurological decline may occur |
|
Respiratory failure or ARDS |
Oxygen therapy, careful respiratory monitoring, and non-invasive or invasive ventilation when required |
Aerosol-generating procedures require airborne precautions and experienced staff |
|
Haemodynamic instability |
Intravenous fluids, vasopressors if required, |
Autonomic dysfunction and shock may occur |
|
Suspected secondary bacterial infection |
Use antibiotics only when clinically indicated |
Avoid routine unnecessary antimicrobial use |
|
Antiviral or antibody-based therapy |
Supportive care remains the mainstay; ribavirin |
Consider investigational therapies only under national or institutional guidance, preferably within clinical trial or monitored compassionate-use frameworks |
|
Healthcare worker protection |
Assign a small, trained team, supervise donning |
Reduces risk of healthcare-associated amplification |
|
Environmental and waste management |
Frequent disinfection of high-touch surfaces, |
Basic IPC practices are critical in resource-limited settings |
|
Contact tracing and monitoring |
Identify household, healthcare, and other exposed contacts; classify exposure risk; monitor |
Public health teams should be involved |
Abbreviations: ARDS, acute respiratory distress syndrome; IPC, infection prevention and control; PPE, personal protective equipment.
Ribavirin has been used empirically during some Nipah virus outbreaks, most notably during the Malaysia outbreak, where it was evaluated in an open-label, non-randomised study of acute Nipah encephalitis. In that study, 140 patients received ribavirin and 54 served as controls, mostly because they were treated before ribavirin became available or declined treatment [28]. Mortality was lower in the ribavirin group than in controls (32% versus 54%), corresponding to a reported 36% reduction in mortality; in Cox regression, ribavirin use was independently associated with better survival, with a relative risk of death of 0.72 (95% CI 0.56–0.93) [28]. However, the study used historical controls, was not randomised, and may have been confounded by differences in timing of care, clinician experience, disease severity, supportive care, and outbreak phase. Subsequent outbreaks in Bangladesh and India have provided limited and inconsistent clinical experience with ribavirin, and no randomised controlled trial has confirmed a survival benefit [29]. Therefore, ribavirin cannot be recommended as proven therapy, although it may be considered only under national or institutional guidance, preferably within a clinical trial or monitored compassionate-use framework.
Other candidate therapies remain investigational. Favipiravir has shown protective effects in animal models, and remdesivir has demonstrated partial protection in non-human primate studies, particularly when administered early [30, 31]. Monoclonal antibodies targeting henipavirus glycoproteins have shown promise in preclinical studies and early-phase human safety studies [32]. Still, clinical efficacy data in patients with confirmed Nipah virus disease remain very limited. These therapies should not replace high-quality supportive care, early isolation, and outbreak control measures. Future clinical trials will need to be designed for small, sporadic outbreaks, where delayed recognition, high mortality, and limited trial infrastructure remain major barriers.
The prognosis of Nipah virus infection remains poor [33]. Case fatality varies across outbreaks but frequently exceeds 60–70%, and some outbreaks have reported mortality rates as high as 90% (Table 2). In Bangladesh, outbreaks during 2001–2004 resulted in an overall mortality of 73% [10]. In Kerala 2018, 21 of 23 identified patients died, 91.3% [16], whereas the smaller Kerala 2023 outbreak had two deaths among six confirmed cases, 33.3% [17]. Poor outcome is associated with severe encephalitis, respiratory failure, delayed recognition, and need for mechanical ventilation [33]. Survivors remain at risk of persistent neurological and functional sequelae.
FUTURE DIRECTIONS
Current research efforts are focused on improving preparedness and clinical management of Nipah virus infection by developing vaccines, rapid diagnostic tests, and targeted antiviral therapies [34]. Several vaccine candidates based on different platforms, including viral vector, protein subunit, and mRNA technologies, are in development and at least one has progressed to early-phase clinical trials and have demonstrated encouraging immunogenicity and safety profiles in preliminary studies [35, 36]. At the same time, advances in diagnostic technologies aim to develop rapid, portable testing platforms that could enable earlier detection of infections during outbreaks, particularly in resource-limited settings where access to specialised laboratories may be limited [37, 38].
Beyond therapeutics and diagnostics, strengthening surveillance systems at the human–animal interface remains a critical priority [39]. Because fruit bats serve as the natural reservoir of the Nipah virus, improved monitoring of viral circulation in bat populations and early identification of spillover events could help detect outbreaks sooner [40, 41]. In parallel, enhancing infection prevention capacity in healthcare facilities, including training of healthcare workers, ensuring availability of personal protective equipment, and establishing clear outbreak response protocols, will remain essential components of preparedness [7]. Together, these measures may improve the ability to detect, manage, and contain future outbreaks of Nipah virus infection.
LIMITATIONS
This review has several limitations that should be considered when interpreting its conclusions. First, as a narrative clinician-oriented review rather than a formal systematic review or meta-analysis, the selection of included studies was not based on a predefined protocol or comprehensive search strategy. Consequently, there is a potential for selection bias, and some relevant studies or emerging data may not have been included.
Second, the available evidence on Nipah virus infection remains limited and heterogeneous. Much of the current knowledge is derived from outbreak investigations, small observational cohorts, and retrospective analyses conducted in specific geographic regions, primarily Bangladesh, India, and Malaysia. These studies vary in methodology, case definitions, and reporting quality, which may limit the comparability and generalizability of findings across different settings.
Third, the relatively small number of reported human cases globally constrains the strength of clinical evidence. Many conclusions regarding clinical presentation, transmission dynamics, and management are based on limited datasets, and in some instances, on expert opinion or extrapolation from related paramyxoviruses. This is particularly relevant for therapeutic interventions, where robust randomized controlled trial data are lacking.
Fourth, diagnostic and surveillance limitations in resource-constrained settings may result in under-recognition and underreporting of cases. As highlighted in the manuscript, laboratory confirmation often requires specialized facilities, and delays in diagnosis may affect both clinical characterization and epidemiological understanding. Therefore, the true burden and spectrum of disease may be incompletely captured.
Fifth, rapidly evolving research on the Nipah virus, including advances in diagnostics, therapeutics, and vaccine development, means that some aspects of this review may become outdated as new evidence emerges. In particular, ongoing clinical trials and experimental therapies may significantly alter future management recommendations.
Finally, this review focuses primarily on clinical aspects relevant to frontline practitioners and does not provide an exhaustive analysis of virological, immunological, or ecological dimensions of Nipah virus infection. While this approach enhances clinical applicability, it may omit important mechanistic insights relevant to a broader scientific audience.
CONCLUSIONS
Nipah virus infection remains an uncommon but highly consequential cause of acute encephalitis and respiratory illness. For clinicians, the key priorities are early recognition of the neuro-respiratory syndrome, awareness of clustering and transmission risk, prompt implementation of infection prevention measures, and aggressive supportive care. Human-to-human transmission, especially in hospitals and households, is now well established in South Asian outbreaks, making early diagnosis and containment critical. As no licensed treatment currently exists, preparedness depends on vigilance, rapid laboratory support, and robust infection control.
Beyond individual patient care, Nipah virus infection represents a broader challenge at the interface of clinical medicine and public health. The combination of high case fatality, potential for nosocomial amplification, and limited therapeutic options underscores the need for integrated outbreak preparedness strategies. Clinicians play a central role not only in recognizing cases but also in triggering early public health responses, including case isolation, contact tracing, and risk communication. In this context, maintaining a high index of suspicion in appropriate epidemiological settings remains essential.
Strengthening healthcare system readiness is equally important. This includes ensuring the availability of personal protective equipment, training healthcare workers in infection prevention and control practices, and establishing protocols for rapid triage and isolation of suspected cases. Laboratory capacity must also be enhanced, with improved access to timely molecular diagnostics and the development of reliable point-of-care tests, particularly in resource-limited settings where outbreaks often occur.
At the same time, advances in research offer cautious optimism. Ongoing efforts to develop vaccines, antiviral agents, and monoclonal antibodies may transform the future management of Nipah virus infection. However, until such interventions become widely available and clinically validated, supportive care and transmission prevention will remain the cornerstones of management.
Finally, a One Health approach that integrates human, animal, and environmental surveillance is critical to reducing the risk of future outbreaks. Improved understanding of spillover dynamics, coupled with community-based interventions to reduce high-risk exposures, may help mitigate the emergence of new cases. In an increasingly interconnected world, the potential for geographic spread beyond currently affected regions reinforces the importance of global preparedness, coordinated surveillance, and sustained investment in research and health system strengthening.
Funding
This work did not receive any specific funding from public, commercial, or not-for-profit funding agencies.
Conflict of interest
The authors declare no conflicts of interest relevant to this article.
Acknowledgements
Alfonso J. Rodriguez-Morales acknowledges the project titled “Caracterización de la epidemiología y carga para la salud pública de enfermedades infecciosas emergentes y re-emergentes en Colombia y Latinoamérica” (Characterisation of the epidemiology and public health burden of emerging and re-emerging infectious diseases in Colombia and Latin America), Código: PE005, at the Institución Universitaria Visión de las Américas. In addition, for his institutional purposes, this article has been registered in the Research Proposal Registration of the Coordination of Scientific Integrity and Surveillance of Universidad Cientifica del Sur, Lima, Peru.
REFERENCES
[1] Ochani RK, Batra S, Shaikh A, Asad A. Nipah virus - the rising epidemic: a review. Infez Med. 2019; 27(2): 117-127.
[2] Rizzardini G, Saporito T, Visconti A. What is new in infectious diseases: Nipah virus, MERS-CoV and the Blueprint List of the World Health Organization. Infez Med. 2018; 26(3): 195-198.
[3] Hassan MZ, Ibrahim SK, Harriss E, et al. Interpreting the natural history and pathogenesis of Nipah virus disease through clinical data, to inform clinical trial design: a systematic review. Lancet Microbe. 2026; 7(4): 101295.
[4] Goh KJ, Tan CT, Chew NK, et al. Clinical features of Nipah virus encephalitis among pig farmers in Malaysia. N Engl J Med. 2000; 342(17): 1229-1235.
[5] Chandni R, Renjith TP, Fazal A, et al. Clinical manifestations of Nipah virus-infected patients who presented to the emergency department during an outbreak in Kerala State in India, May 2018. Clin Infect Dis. 2020; 71(1), 152-157.
[6] Chadha MS, Comer JA, Lowe L, et al. Nipah virus-associated encephalitis outbreak, Siliguri, India. Emerg Infect Dis. 2006; 12(2): 235-240.
[7] Pritchard S, Hornsey E. The role of infection prevention and control in the mitigation of human-to-human transmission of Nipah virus: a systematic review. Antimicrob Resist Infect Control. 2025; 15(1): 1.
[8] Banerjee S, Gupta N, Kodan P, et al. Nipah virus disease: a rare and intractable disease. Intractable Rare Dis Res. 2019; 8(1): 1-8.
[9] Chong HT, Kunjapan SR, Thayaparan T, et al. Nipah encephalitis outbreak in Malaysia, clinical features in patients from Seremban. Can J Neurol Sci. 2002; 29(1): 83-87.
[10] Hossain MJ, Gurley ES, Montgomery JM, et al. Clinical presentation of Nipah virus infection in Bangladesh. Clin Infect Dis. 2008; 46(7): 977-984.
[11] Satter SM, Rahman DI, Sultana S, et al. Epidemiology, clinical characteristics, and genetic diversity of Nipah virus strains from Bangladesh: 2016-2023. Int J Infect Dis. 2025; 159: 108010.
[12] Yeasmin D, Hossain MM, Haider S, et al. The deadly drink: Nipah virus transmission through date palm sap, cultural practices and the evolution of behavioral interventions in Bangladesh over two decades. J Infect Public Health. 2025; 18: 102949.
[13] Jackson J, Shanta IS, McKee C, et al. Identifying weather patterns affecting household date palm sap consumption in Bangladesh, 2013-2016. PLoS One. 2024; 19(12): e0313904.
[14] Anish TS, Aravind R, Radhakrishnan C, et al. Pandemic potential of the Nipah virus and public health strategies adopted during outbreaks: lessons from Kerala, India. PLOS Glob Public Health. 2024; 4(12): e0003926.
[15] Sun YQ, Zhang YY, Liu MC, et al. Mapping the distribution of Nipah virus infections: a geospatial modelling analysis. Lancet Planet Health. 2024; 8(7): e463-e475.
[16] Pallivalappil B, Ali A, Thulaseedharan N, et al. Dissecting an outbreak: a clinico-epidemiological study of Nipah virus infection in Kerala, India, 2018. J Glob Infect Dis. 2020; 12(1): 21-27.
[17] Anoop Kumar AS, Sahay RR, Radhakrishnan C, et al. Clinico-epidemiological presentations and management of Nipah virus infection during the outbreak in Kozhikode district, Kerala state, India 2023. J Med Virol. 2024; 96(2): e29559.
[18] Nikolay B, Salje H, Hossain MJ, et al. Transmission of Nipah virus - 14 years of investigations in Bangladesh. N Engl J Med. 2019; 380(19): 1804-1814.
[19] Lim CCT, Lee WL, Leo YS, et al. Late clinical and magnetic resonance imaging follow up of Nipah virus infection. J Neurol Neurosurg Psychiatry. 2003; 74(1): 131-133.
[20] Ng BY, Lim CCT, Yeoh A, Lee WL. Neuropsychiatric sequelae of Nipah virus encephalitis. J Neuropsychiatry Clin Neurosci. 2004; 16(4): 500-504.
[21] Aquib WR, Mondal UK, Nazneen A, et al. Long-term sequelae and functional outcomes in the largest cohort of Nipah virus survivors in Bangladesh. Lancet Reg Health Southeast Asia. 2026; 45: 100729.
[22] Gupta N, Nischal N. Management of acute febrile diseases in limited resource settings: a case-based approach. Infez Med. 2020; 28(1): 11-16.
[23] Cárdenas G, Salgado P, Laura-Foronda E, et al. Neglected and (re-)emergent infections of the CNS in low-/middle-income countries. Infez Med. 2021; 29(4): 513-525.
[24] Bhatt M, Soneja M, Gupta N. Approach to acute febrile illness during the COVID-19 pandemic. Drug Discov Ther. 2021; 14(6): 282-286.
[25] Mazzola L, Fru HC, Cherkaoui D, et al. Diagnostic tests for Nipah virus: a landscape analysis. Diagn Microbiol Infect Dis. 2026; 114(1): 117101.
[26] Sahay RR, Patil DY, Shete AM, et al. Rapidly deployable mobile BSL-3 laboratory: a response to the Nipah virus outbreak in Kozhikode, Kerala, India, 2023. Pathog Glob Health. 2025; 119: 1-10.
[27] Hassan MZ, Rojek A, Olliaro P, Horby P. Improving clinical care of patients in Nipah outbreaks: moving beyond compassionate use. Lancet Reg Health Southeast Asia. 2025; 33: 100527.
[28] Chong HT, Kamarulzaman A, Tan CT, et al. Treatment of acute Nipah encephalitis with ribavirin. Ann Neurol. 2001; 49(6): 810-813.
[29] Chan XHS, Haeusler IL, Choy BJK, et al. Therapeutics for Nipah virus disease: a systematic review to support prioritisation of drug candidates for clinical trials. Lancet Microbe. 2025; 6, 101002.
[30] Dawes BE, Kalveram B, Ikegami T, et al. Favipiravir (T-705) protects against Nipah virus infection in the hamster model. Sci Rep. 2018; 8(1): 7604.
[31] de Wit E, Williamson BN, Feldmann F, et al. Late remdesivir treatment initiation partially protects African green monkeys from lethal Nipah virus infection. Antiviral Res. 2023; 216: 105658.
[32] Playford EG, Munro T, Mahler SM, et al. Safety, tolerability, pharmacokinetics, and immunogenicity of a human monoclonal antibody targeting the G glycoprotein of henipaviruses in healthy adults: a first-in-human, randomised, controlled, phase 1 study. Lancet Infect Dis. 2020; 20(4): 445-454.
[33] Alla D, Shah DJ, Adityaraj N, et al. A systematic review of case reports on mortality, modes of infection, diagnostic tests, and treatments for Nipah virus infection. Medicine (Baltimore). 2024; 103(44): e39989.
[34] Moore KA, Mehr AJ, Ostrowsky JT, et al. Measures to prevent and treat Nipah virus disease: research priorities for 2024-29. Lancet Infect Dis. 2024; 24(11): e707-e717.
[35] Kim S, Kang H, Skrip L, et al. Progress and challenges in Nipah vaccine development and licensure for epidemic preparedness and response. Expert Rev Vaccines. 2025; 24(1): 183-193.
[36] Frenck RW, Naficy A, Feser J, et al. Safety and immunogenicity of a Nipah virus vaccine (HeV-sG-V) in adults: a single-centre, randomised, observer-blind, placebo-controlled, phase 1 study. Lancet. 2025; 406: 2792-2803.
[37] Miao J, Zuo L, He D, et al. Rapid detection of Nipah virus using the one-pot RPA-CRISPR/Cas13a assay. Virus Res. 2023; 332: 199130.
[38] Pollak NM, Olsson M, Marsh GA, et al. Evaluation of three rapid low-resource molecular tests for Nipah virus. Front Microbiol. 2023; 13: 1101914.
[39] Satter SM, Aquib WR, Sultana S, et al. Tackling a global epidemic threat: Nipah surveillance in Bangladesh, 2006-2021. PLoS Negl Trop Dis. 2023; 17(9): e0011617.
[40] Deshpande K, Vanak AT, Devy MS, Krishnaswamy J. Forbidden fruits? Ecosystem services from seed dispersal by fruit bats in the context of latent zoonotic risk. Oikos. 2022; 2022(1): e08359.
[41] Balasubramanian R, Mohandas S, Thankappan UP, et al. Surveillance of Nipah virus in Pteropus medius of Kerala state, India, 2023. Front Microbiol. 2024; 15: 1342170.