Le Infezioni in Medicina, n. 2, 144-149, 2026
REVIEWS
HIV-2 infection in Europe – persistence by migrant flows from West Africa but low spillover into the native population
Vicente Soriano1, María del Carmen Nieto2, Ana Belén Lozano3, María José Pena4,5, José Manuel Ramos6, Sonia Algarate7, Ariadna Rando8, Víctor Moreno-Torres9, Pablo Barreiro10, Carmen de Mendoza9
1 UNIR Health Sciences School, Universidad Internacional de La Rioja, Madrid, Spain;
2 Microbiology Department, Hospital Universitario de Basurto, Bilbao, Spain;
3 Internal Medicine Department, Hospital de Poniente, Almería, Spain;
4 Microbiology Department, Hospital Universitario Dr. Negrín, Las Palmas, Spain;
5 Instituto de Investigación Sanitaria de Canarias, Las Palmas, Spain;
6 Internal Medicine, Hospital Universitario Dr. Balmis, Alicante, Spain;
7 Microbiology Department, Hospital Clínico Universitario Lozano Blesa, Zaragoza, Spain;
8 Microbiology Department, Hospital Universitari Vall d’ Hebrón, Barcelona, Spain;
9 Internal Medicine Department, Puerta de Hierro University Hospital, Madrid, Spain;
10 Infectious Diseases Unit, La Paz University Hospital, Madrid, Spain.
Article received 20 February 2026 and accepted 14 April 2026
Corresponding author
Vicente Soriano
E-mail: vicente.soriano@unir.net
SUMMARY
HIV-2 was isolated in 1986 in AIDS patients with negative or indeterminate HIV-1 antibodies. Most HIV-2 patients initially reported were West African migrants living in Europe. Independence wars during the 1960s for French colonies and, in the 1970s, for Portuguese colonies, fueled population exchanges, including military personnel. The Ivory Coast and Guinea-Bissau acted as the respective epicenters of HIV-2 spillover into France and Portugal. Other European countries (i.e., Belgium, the Netherlands, Spain, Italy, Germany, etc.) reported HIV-2 cases in the late 1980s. Although the majority were migrants from West Africa, there were also natives who had traveled to or had sex partners from there. By 1990, nearly 500 cases of HIV-2 infection had been confirmed in Europe. By 2010, nearly 2,000 cases had been reported only in Portugal.
National surveillance data across Europe remain scarce, hindering precise and up-to-date estimates of HIV-2 infection. Spain is a notable exception, as it has maintained a register since 1989, with 428 HIV-2 cases reported by the end of 2025. Current consensus indicates that new HIV-2 infections are declining across Europe. Migrants from West Africa continue to be the largest contributors, with no evidence of significant HIV-2 spread into the native European population. This ongoing pattern underscores both the importance of surveillance and the limited transmission of HIV-2 beyond migrant communities.
Keywords: HIV-2, AIDS, West Africa, Europe, migrants, antiretroviral therapy, HIV-1 coinfection.
INTRODUCTION
Human immunodeficiency virus type 2 (HIV-2) was first isolated in 1986 in patients with AIDS in whom the serology for HIV-1 was negative or indeterminate [1]. Circulation of a virus closely related but distinct from HIV-1 had been suspected for a while in West Africa [2]. The complete genome sequence of HIV-2 was reported in 1987 and showed 55% nucleotide divergence from HIV-1 [3]. Individuals with HIV-2 infection began to be reported in France and Portugal, and surveys in their former West African colonies suggested that the virus was widely circulating there [4-6].
Viral replication in individuals with HIV-2 infection is lower than in HIV-1 carriers [7, 8]. It results in slower CD4 count decline, lower transmissibility, delayed progression to AIDS, and lower mortality in HIV-2 compared to HIV-1 infection [9]. Approximately 10% of individuals with HIV-2 infection are classified as ‘elite controllers’ [10]. They show undetectable viremia and CD4 counts above 500 cells/mm3 after more than 10 years of infection, even without antiretroviral therapy.
In an early reconstruction of HIV-2’s spread into Europe, nearly 500 cases had been confirmed by 1990 [11]. Most were reported in France and Portugal, and the majority were linked to former West African colonies. Ivory Coast and Senegal were the primary sources of HIV-2 infections for France [5, 11, 12]. Guinea-Bissau was the epicenter for HIV-2 cases identified in Portugal [6, 13, 14]. Significant migrant flows, including military personnel during the independence wars in the 1960s and 1970s, fueled the initial European spread of HIV-2 [15, 16].
In this narrative review, we aim to update about the current circulation of HIV-2 infection in Europe and discuss epidemiological trends. We provide insights and future prospects for the HIV-2 epidemics in Europe after deeper examination of the situation in Spain, using a nationwide database of HIV-2 cases. The searching methodology was based on articles published in PubMed during the last four decades, including the word ‘HIV-2’ and resembling expressions.
HIV-2 in France
In France, HIV-2 infections were examined in new HIV diagnoses twenty years ago [17]. From a total of 10,184 new HIV-infected individuals reported over three years, 186 (1.8%) were infected with HIV-2. Coinfection with HIV-1 was found in 22 of them. The serological diagnosis of dual infection was based on similar high antibody binding affinity to the respective immunodominant epitopes of the transmembrane protein [18, 19].
Up to 65% of individuals infected with HIV-2 (n=121) diagnosed in France had been born in West Africa, mainly Côte d’Ivoire (n=64), Mali (n=19), and Senegal (n=12). There were also 20 native French individuals [17]. Women represented 63% of HIV-2 cases. The risk factor was unknown for 26%, but heterosexual transmission was the most likely route for 72%. In three males, homosexual transmission was well documented. No more nationwide surveys have reported updated HIV-2 figures in France; current estimates are a few thousand.
HIV-2 in Portugal
The cumulative number of notified HIV-2 infections in Portugal was 1,813 by the end of 2008 [16]. Until the year 2000, the majority of HIV-2 patients were Portuguese-born males living in the north of the country. In contrast, from 2000 to 2007, most individuals diagnosed with HIV-2 infection in Portugal had a West African origin, were predominantly female and were living in the capital, Lisbon. Movements of soldiers and repatriates from African territories during the independence wars and, later, migration and mobility from HIV-2 highly endemic areas largely determined such different patient profiles [20, 21].
The role of Guinea-Bissau as the epicenter for the global HIV-2 spreading throughout Portuguese ties has been well documented [6, 14, 16]. Founder effects for HIV-2 in Brazil and India seem to be a direct consequence of this link [22, 23].
HIV-2 infection in other European countries
A short case series of HIV-2 patients has been reported in Italy. Until 2020, a large clinic in northern Italy reported 32 cases, 84% of which were of African origin. Half of them were male. HIV-2 viremia was undetectable in 37% of cases. Nearly half were dual HIV-1/HIV-2 infections. Heterosexual transmission was the most frequent route of contagion [24].
In the Netherlands, earlier reports of HIV-2 infection referred to West African migrants living near the Rotterdam port [25]. A more recent study noticed that less than 4% of people with HIV in the country had been diagnosed with HIV-2 infection [10]. To date, the Rotterdam cohort has included 52 HIV-2 patients, of whom 27 keep on regular follow-up [10]. Over 80% are African, most from Cape Verde.
In Belgium and Luxembourg, 65 HIV-2 patients were virologically characterized two decades ago, being the majority West African migrants. Other European countries that have reported HIV-2 cases are Germany and the United Kingdom, again, with most of them being West Africans [26-28].
The Spanish HIV-2 register
The first cases of HIV-2 infection in Spain were reported in 1988 in two migrants from Senegal and one from Gambia living in Barcelona [29]. A national register of HIV-2 cases was then created. Yearly meetings have been arranged to update information on new HIV-2 diagnoses and longitudinal follow-up when possible [30]. A centralized laboratory performs subtyping, viral load and drug resistance testing for HIV-2 [31].
Up to the end of 2025, a total of 428 cases of HIV-2 infection had been reported in Spain. A total of 331 (77.4%) were Sub-Saharan Africans, being native Spaniards only 59 (13.8%). The mean age at diagnosis was 42 years, ranging from newborns to 83 years-old. Male were more common than women, being 271 (63.5%). Heterosexual transmission was the most likely route of infection for 289 (67.7%). There were 5 cases attributable to blood transfusions, 3 to vertical transmission, 6 to injection drug use, and 15 to male homosexual contacts. HIV-1 and HIV-2 coinfection was demonstrated in 39 (9.1%). Longitudinal follow-up was available for 123 HIV-2 individuals. Their median CD4 count was 568 cells/mm3. Ten (11.7%) had less than 200 cells/mm3. Antiretroviral therapy with tenofovir/emtricitabine plus integrase inhibitors, either dolutegravir or bictegravir, was taken by 79% of patients, being the remaining 21% treated with boosted darunavir. Undetectable viral load was recognized in 87% of patients.
The annual incidence of HIV-2 in Spain has declined after peaking 15 years ago [32]. The current number of incident cases is around 10 per year. We can recognize three periods in the reporting of HIV-2 in Spain during the last four decades (Figure 1).
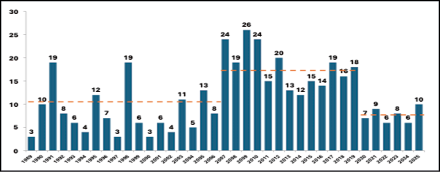
Figure 1 - Number of yearly new diagnoses of HIV-2 infection in Spain.
Before 2006, the average annual incidence was 11 cases. It then rose to an average of 20 cases annually until the COVID-19 pandemic. The increase largely resulted from the arrival of African migrants to the Canary Islands and southeastern Spanish coasts during that period. Since 2020, fewer than ten HIV-2 cases per year have been reported in Spain. We suggest that early identification of HIV-2 in newcomers, combined with declining HIV-2 rates in their countries of origin, largely explains the current low incidence in Spain, with very few or only occasional local transmissions.
Of all 428 cumulative cases of HIV-2 reported to date, 330 (77.3%) are Sub-Saharan Africans. Being a country of 50 million people, Spain has 7 million foreigners (14%). Roughly 250,000 are Sub-Saharan Africans, with West Africans being the largest group by far. Migrants from this region are mostly from Senegal (75,000), Nigeria (35,000), Mali (30,000), Ghana (20,000) and Equatorial Guinea (10,000) [33]; the latter is a former Spanish colony (Figure 2).
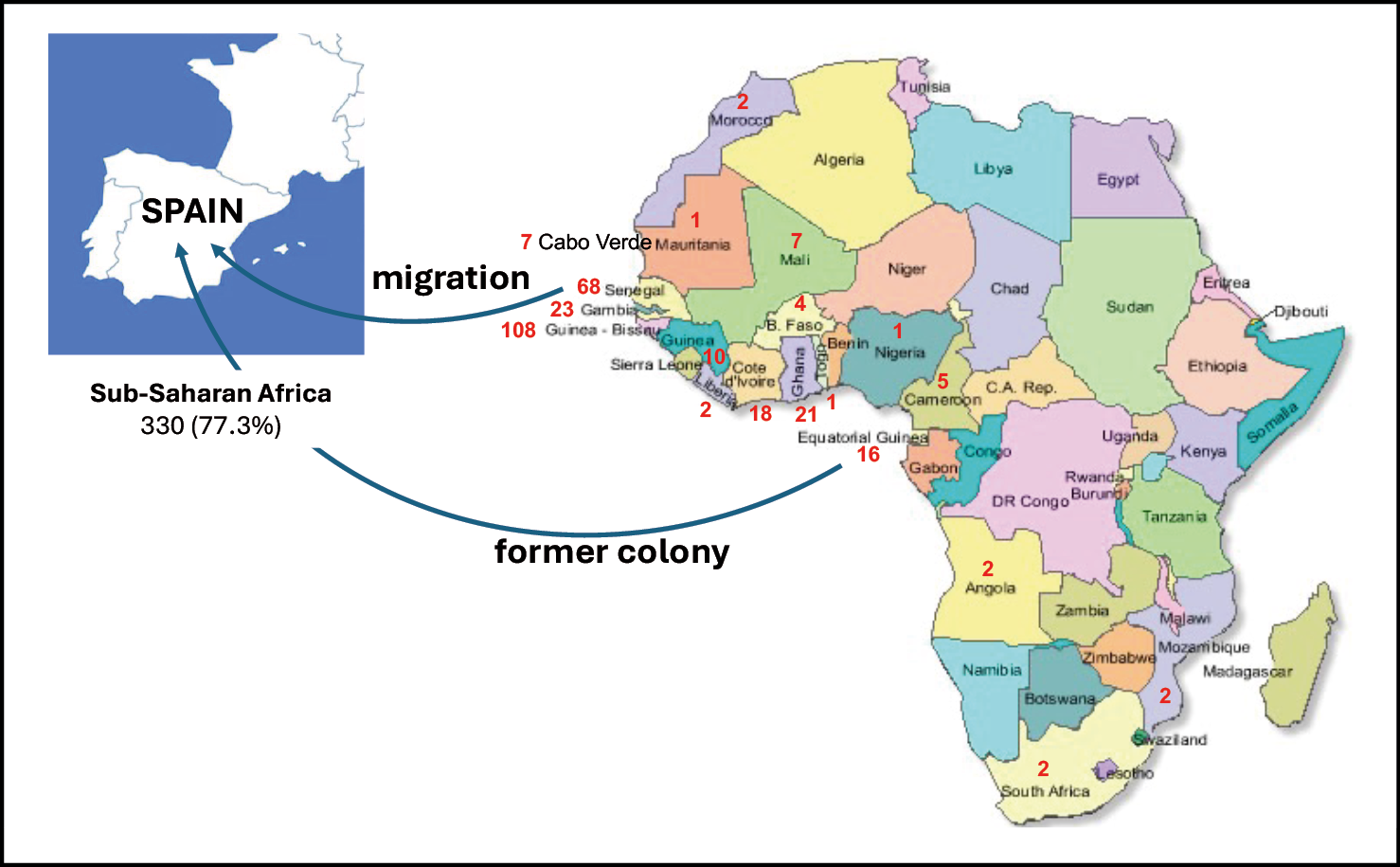
Figure 2 - The country of origin for individuals with HIV-2 infection reported in Spain.
Future trends for HIV-2 in Europe
Europe was the first region where HIV-2 patients were identified among West African migrants, yet the infection remains largely neglected [34]. Notably, France and Portugal continue to have the largest numbers of HIV-2 carriers. However, national surveillance data are generally scarce, making it difficult to provide precise and updated estimates of HIV-2 infection in Europe. Spain stands out as an exception, maintaining a register since 1989 and reporting 428 cases of HIV-2 infection by the end of 2025. These surveillance differences impact the ability to fully understand the epidemic’s scope.
Heterosexual transmission has been and continues to be the most frequent route of acquisition of HIV-2 in Europe as elsewhere [9]. In contrast with HIV-1, men having sex with men only sporadically have been reported as infected with HIV-2, including a cluster of eight older men in Spain [35]. Contrary to HIV-1, perinatal transmission of HIV-2 is naturally uncommon [36]. No recent reports of vertical transmission of HIV-2 from European countries have been released. Universal perinatal HIV-1/2 testing along with antiretroviral coverage during pregnancy, have driven to almost zero any chance of mother to child transmission of HIV-2.
Consensus exists that new HIV-2 infections in Europe are decreasing [10, 21, 24, 26, 32]. Migrants from West Africa remain the primary source of cases, with no significant ongoing transmission within the native population. This contrasts with HIV-1, a more transmissible zoonosis from central Africa, which spread from the beginning widely among Europeans. While HIV-1 rapidly established itself within the native population upon arrival, new HIV-2 diagnoses continue to occur mostly among migrants from endemic West African countries. Strengthened medical management of HIV-2 infected individuals should further prevent the spread across Europe and help controlling the epidemic [37]. Furthermore, encouraging recent data from West African countries highlight that HIV-2 circulation is rapidly declining there [38-40].
Funding
This work was supported in part by grants UNIR-ITEI, no. I25-003; ISCIII-FIS, PI21/1717 and PI24/1996.
Conflict of interets
None for all authors.
REFERENCES
[1] Clavel F, Guétard D, Brun-Vézinet F, et al. Isolation of a new human retrovirus from West African patients with AIDS. Science. 1986; 233: 343-346.
[2] Barin F, M’Boup S, Denis F, et al. Serological evidence for virus related to simian T-lymphotropic retrovirus III in residents of West Africa. Lancet. 1985; 2: 1387-1389.
[3] Guyader M, Emerman M, Sonigo P, Clavel F, Montagnier L, Alizon M. Genome organization and transactivation of the human immunodeficiency virus type 2. Nature. 1987; 326: 662-669.
[4] Clavel F, Mansinho K, Chamaret S, et al. Human immunodeficiency virus type 2 infection associated with AIDS in West Africa. N Engl J Med. 1987; 316: 1180-1185.
[5] Odehouri K, De Cock K, Krebs J, Moreau J, Rayfield M, McCormick J, Schochetman G, Bretton R, Bretton G, Ouattara D, et al. HIV-1 and HIV-2 infection associated with AIDS in Abidjan, Côte d’Ivoire. AIDS 1989; 3: 509-512.
[6] Faria N, Hodges-Mameletzis I, Silva JC, ET AL. Phylogeographical footprint of colonial history in the global dispersal of human immunodeficiency virus type 2 group A. J Gen Virol. 2012; 93: 889-899.
[7] Simon F, Matheron S, Tamalet C, et al. Cellular and plasma viral load in patients infected with HIV-2. AIDS. 1993; 7: 1411141-1411147.
[8] Shanmugam V, Switzer W, Nkengasong J, et al. Lower HIV-2 plasma viral loads may explain differences between the natural histories of HIV-1 and HIV-2 infections. J Acquir Immune Defic Syndr. 2000; 24: 257-263.
[9] De Cock K, Adjorlolo G, Ekpini E, et al. Epidemiology and transmission of HIV-2. Why there is no HIV-2 pandemic. JAMA. 1993; 270: 2083-2086.
[10] Hensley K, Gruters R, van Nood E, ET AL. Insights to a cure: unique controller phenotypes in the Rotterdam HIV-2 Cohort. Open Forum Infect Dis. 2025; 12: ofaf336.
[11] Smallman-Raynor M, Cliff A. The spread of human immunodeficiency virus type 2 into Europe: a geographical analysis. Int J Epidemiol. 1991; 20: 480-409.
[12] Brun-Vezinet F, Rey MA, Katlama C, et al. Lymphadenopathy-associated virus type 2 in AIDS and AIDS-related complex. Clinical and virological features in four patients. Lancet. 1987; 1: 128-132.
[13] Soriano V, Gomes P, Heneine W, ET AL. Human immunodeficiency virus type 2 (HIV-2) in Portugal: clinical spectrum, circulating subtypes, virus isolation, and plasma viral load. J Med Virol. 2000; 61: 111-116.
[14] Varanda J, Santos JM. It was not the perfect storm: the social history of the HIV-2 virus in Guinea-Bissau. Trop Med Infect Dis. 2023; 8: 261.
[15] Saal F, Sidibe S, Alves-Cardoso E, et al. Anti HIV-2 serological screening in Portuguese populations native from or having had close contact with Africa. AIDS Res Hum Retroviruses. 1987; 3: 341-342.
[16] Carvalho AC, Valadas E, França L, et al. Population mobility and the changing epidemics of HIV-2 in Portugal. HIV Med. 2012; 13: 219-225.
[17] Barin F, Cazein F, Lot F, et al. Prevalence of HIV-2 and HIV-1 group O infections among new HIV diagnoses in France: 2003-2006. AIDS. 2007; 21: 2351-2353.
[18] Baillou A, Janvier B, Leonard G, Denis F, Goudeau A, Barin F. Fine serotyping of human immunodeficiency virus serotype 1 (HIV-1) and HIV-2 infections by using synthetic oligopeptides representing an immunodominant domain of HIV-1 and HIV-2/simian immunodeficiency virus. J Clin Microbiol. 1991; 29: 1387-1391.
[19] Soriano V, Gutiérrez M, Heredia A, et al. Serial dilutions on synthetic peptide-based assays can resolve dual seroreactivity to HIV-1 and HIV-2. Vox Sang. 1996; 71: 67-68.
[20] Lemey P, Pybus O, Wang B, Saksena M, Salemi M, Vandamme AM. Tracing the origin and history of the HIV-2 epidemic. Proc Natl Acad Sci USA. 2003; 100: 6588-6592.
[21] Valadas E, França L, Sousa S, Antunes F. 20 years of HIV-2 infection in Portugal: trends and changes in epidemiology. Clin Infect Dis. 2009; 48: 1166-1167.
[22] Cortes E, Detels R, Aboulafia D, Li X, Moudgil T, Alam M, Bonecker C, Gonzaga A, Oyafuso L, Tondo M. HIV-1, HIV-2, and HTLV-I infection in high-risk groups in Brazil. N Engl J Med. 1989; 320: 953-958.
[23] Tiewsoh J, Antony B, Boloor R. Seroprevalence of HIV-2 and dual infection among HIV-infected individuals with clinical and laboratory features at a Tertiary Care Teaching Hospital, Mangalore: The present scenario. Ann Afr Med. 2019; 18: 70-74.
[24] Fumarola B, Calza S, Renzetti S, et al. Immunological evolution of a cohort of HIV-2 infected patients: peculiarities of an underestimated infection. Mediterr J Hematol Infect Dis. 2022; 14: e2022016.
[25] van der Ende ME, Schutten M, Ly T, Gruters R, Osterhaus A. HIV-2 infection in 12 European residents: virus characteristics and disease progression. AIDS. 1996; 10:1649-1655.
[26] Ruelle J, Roman F, Vandenbroucke AT, et al. Transmitted drug resistance, selection of resistance mutations and moderate antiretroviral efficacy in HIV-2: analysis of the HIV-2 Belgium and Luxembourg database. BMC Infect Dis. 2008; 8: 21.
[27] Marquart K, Muller H, Brede H. HIV-2 in West Germany. AIDS 1988; 2: 141.
[28] Evans B, Gill O, Gleave S. HIV-2 in the United Kingdom - A review. CDR. 1991; 1: R19-R23.
[29] Soriano V, Tor J, Ribera A. Human immunodeficiency virus type 2 in Spain. Eur J Clin Microbiol Infect Dis. 1989; 8: 568.
[30] de Mendoza C, Cabezas T, Caballero E, et al. Spanish HIV-2 Network. HIV type 2 epidemic in Spain: challenges and missing opportunities. AIDS. 2017; 31: 1353-1364.
[31] Treviño A, de Mendoza C, Caballero E, et al. HIV-2 Spanish Study Group. Drug resistance mutations in patients infected with HIV-2 living in Spain. J Antimicrob Chemother. 2011; 66: 1484-1488.
[32] de Mendoza C, Lozano AB, Rando A, et al. Spanish HIV-2 Network. The incidence of HIV-2 infection in Spain is declining - a registry data analysis. Int J Infect Dis. 2024; 146: 107076.
[33] Instituto Nacional de Estadística (INE). https://www.ine.es/buscar/searchResults.do?searchString=Estadística+de+Migraciones&Menu_botonBuscador=&searchType=DEF_SEARCH&startat=0&L=0 (accessed February 15th 2026)
[34 Ceccarelli G, Giovanetti M, Sagnelli C, et al. Human immunodeficiency virus type 2: the neglected threat. Pathogens. 2021; 10: 1377.
[35] Cilla G, Rodés B, Pérez-Trallero E, Arrizabalaga J, Soriano V. Molecular evidence of homosexual transmission of HIV type 2 in Spain. AIDS Res Hum Retroviruses. 2001; 17: 417-422.
[36] Ter Schiphorst E, Hansen K, Holm M, Hønge B. Mother-to-child HIV-2 transmission: comparison with HIV-1 and evaluation of factors influencing the rate of transmission. A systematic review. Trans R Soc Trop Med Hyg. 2022; 116: 399-408.
[37] Gottlieb G, Raugi D, Smith R. 90-90-90 for HIV-2? Ending the HIV-2 epidemic by enhancing care and clinical management of patients infected with HIV-2. Lancet HIV 2018; 5: e390-399.
[38] Fryer H, Van Tienen C, Van Der Loeff M, et al. Predicting the extinction of HIV-2 in rural Guinea-Bissau. AIDS. 2015; 29: 2479-2486.
[39] Konan B, de Mendoza C, Kouadio CH, et al. The burden of HIV-1 and HIV-2 epidemics in Ivory Coast. AIDS Rev. 2024; 26: 151-157.
[40] De Mendoza C, Soriano V. Is the HIV-2 pandemic vanishing? AIDS Rev. 2025; 27: 68-69.