Le Infezioni in Medicina, n. 2, 131-143, 2026
REVIEWS
Imported Leishmaniasis in Europe (2000-2024): A systematic review of travel-related case reports
Sandra M. Alcocer-Veintimilla1, Víctor A. Pillajo-Gangotena1, Jaime David Acosta-España2,3,4,5,6, Aula Abbara7, Marta González-Sanz8,9, Alfonso J. Rodriguez-Morales10
1 School of Medicine, Health Sciences Faculty, Universidad Internacional SEK del Ecuador, Quito, Ecuador;
2 Microbiology, Infectious Diseases and Travel Medicine Department, Health Sciences Faculty, Universidad Internacional SEK (UISEK), Quito, Ecuador;
3 Microbiology Department, School of Medicine, Facultad de Salud y Bienestar (FASABI), Pontificia Universidad Católica del Ecuador, Quito, Ecuador;
4 Clinical Medicine, Ribeirão Preto Medical School (FMRP), University of São Paulo, Ribeirão Preto, Sao Paulo, Brazil;
5 Research Group of Emerging and Neglected Diseases, Ecoepidemiology and Biodiversity, Health Sciences Faculty, Universidad Internacional SEK (UISEK), Quito, Ecuador;
6 Centro de Investigación para la Salud en América Latina (CISeAL), Pontificia Universidad Católica del Ecuador, Quito, Ecuador;
7 Faculty of Medicine, Imperial College London, St Mary’s Hospital, London, United Kingdom;
8 National Referral Unit for Tropical Diseases, Infectious Diseases Department, Ramón y Cajal University Hospital, IRYCIS, Madrid, Spain;
9 Universidad de Alcalá, Madrid, Spain;
10 Faculty of Health Sciences, Universidad Científica del Sur, Lima, Perú.
Article received 19 February 2026 and accepted 11 May 2026
Corresponding author
Jaime David Acosta-España
E-mail: jaime.acosta@uisek.edu.ec
SUMMARY
Background: This review aims to systematically analyze imported leishmaniasis cases reported between 2000 and 2024, focusing on geographic origin, host demographics, clinical manifestations, diagnostic approaches, and species distribution.
Methods: A systematic review was conducted in accordance with the PRISMA guidelines across PubMed, Scopus, and Web of Science. Inclusion criteria encompassed case reports and series in English or Spanish that described laboratory-confirmed human leishmaniasis acquired outside of Europe. The risk of bias was assessed using the JBI Critical Appraisal Tool. Data was extracted and analyzed using RStudio (v4.3.1) for statistical exploration, including subgroup analysis and temporal trends. The protocol was registered in PROSPERO (CRD420251128116).
Results: Twelve studies documenting 127 published cases were reviewed, mainly from Germany, Spain, Poland, and Austria. The most common form was cutaneous leishmaniasis (63%), followed by mucocutaneous (27%) and visceral (10%). Visceral leishmaniasis was significantly linked to lower odds of being a tourist (OR: 0.24; 95% CI: 0.07-0.87; p = 0.027). Diagnostic methods varied, including PCR, histology, and microscopy. The main species were L. braziliensis, L. panamensis, and L. donovani. Treatments involved liposomal amphotericin B and systemic antimonials, though resistance and outcomes were inconsistently reported.
Conclusions: The importation of leishmaniasis in Europe highlights a growing health challenge. Diagnostic variability, underreporting, and limited clinician awareness cause delays and mismanagement. Enhancing surveillance, standardizing diagnostics, and adding pre-travel advice to routine care are vital. Future research should focus on species resistance, coinfections, and long-term effects for better guidelines.
Keywords: Leishmaniasis, travel medicine, Europe, systematic review, tourism, Leishmania.
INTRODUCTION
Leishmaniasis is a vector-borne parasitic disease caused by protozoa of the genus Leishmania, transmitted to humans through the bite of infected female sand flies, Phlebotomus species in the Old World (Europe, Asia, and Africa) and Lutzomyia species in the New World (Americas) [1, 2]. It is classified by the World Health Organization as a Neglected Tropical Disease (NTD), reflecting its disproportionate burden on impoverished populations and the limited investment in research, prevention, and treatment compared to other infectious diseases [3].
Clinically, leishmaniasis presents in three primary forms: cutaneous (CL), mucocutaneous (ML), and visceral (VL). CL, the most prevalent form, manifests as ulcerative skin lesions and is caused by species such as L. tropica, L. major, and L. infantum in the Old World, and L. braziliensis, L. mexicana, L. amazonensis, L. guyanensis, and L. panamensis in the New World. ML, primarily associated with L. braziliensis, leads to destructive inflammation of mucosal tissues. VL, the most severe form, affects internal organs such as the spleen, liver, and bone marrow, and is caused by L. donovani and L. infantum (also known as L. chagasi in Latin America, now generally considered synonymous) [1, 3-6].
According to the World Health Organization (WHO), more than 12 million people are currently infected with leishmaniasis, with an estimated 600,000 to 1 million new cases of CL and 50,000 to 90,000 new VL cases annually. It is essential to distinguish the different clinical forms of the disease, which vary markedly in presentation and severity. However, these figures are likely underestimated due to underreporting and limited surveillance in endemic regions [7]. The disease is endemic in 99 countries, with high-risk areas including South Asia, the Middle East, Northeastern Africa, Southern Europe, Latin America, and parts of the southern United States [8, 9]. CL is widespread across the Americas, the Mediterranean basin, the Middle East, and Central Asia. ML is confined mainly to Bolivia, Brazil, Ethiopia, and Peru, and VL is most prevalent in India, South Sudan, Sudan, Brazil, Ethiopia, and Somalia [10].
In Europe, endemic transmission has been reported in Albania, Montenegro, Malta, Greece, Spain, North Macedonia, Italy, and Portugal. In 2024, the WHO documented 133 imported cases of CL and 73 of VL in Europe alone [9, 11]. However, the European epidemiological situation remains poorly understood because not all endemic nations have implemented robust surveillance systems, hence failing to collect and report accurate data. Spain, despite its well-documented endemic transmission, shows how reporting gaps can mask the true epidemiological picture and make regional comparisons more difficult. When endemic countries are missing or only partly represented, the European picture becomes broken, which limits the ability to predict outbreaks and efficiently allocate resources [12].
Environmental changes, particularly those driven by climate change, are reshaping the global distribution of leishmaniasis. Rising temperatures, altered precipitation patterns, deforestation, and urban expansion have expanded the ecological range of sand fly vectors, facilitating transmission in previously non-endemic regions [13, 14]. Sand flies are increasingly found in dry, hot, low-altitude environments, where they utilize rodent burrows, bird nests, and stables as breeding habitats [15]. Modeling studies suggest that climate-driven shifts in vector distribution may significantly increase the population at risk in temperate zones over the coming decades [15].
International travel has become a factor in the global spread of Leishmania species [16]. This poses diagnostic and public health challenges, especially when novel species are introduced into regions with existing endemicity [5]. Surveillance data from European travel clinics have highlighted the increasing frequency of imported cases, often linked to adventure tourism, military deployment, or migration [6, 14].
Despite its growing relevance, leishmaniasis remains an uncommon diagnosis in European clinical settings. Many returning travelers are unaware of their risk of exposure, and clinicians may overlook the disease in their differential diagnoses. Delayed or missed diagnoses are not uncommon, particularly in cases with atypical presentations or long incubation periods. Comprehensive pre-travel consultations, including risk assessment, education, and vector avoidance strategies, are essential for prevention. Accurate diagnosis requires detailed medical and travel history, often extending months or years before symptom onset [6, 13, 14]. This study aims to analyze the epidemiological characteristics of leishmaniasis cases diagnosed in Europe, with a specific focus on imported infections. We hypothesize that the majority of these cases are associated with travel to endemic regions, particularly in the Americas, and that active tourism plays a significant role in the importation of diseases.
METHODS
This systematic review was conducted to identify and analyze epidemiological, clinical, and diagnostic characteristics of imported human leishmaniasis cases reported and diagnosed among travelers from Europe. The review explicitly examines the country of exposure, the country of diagnosis, patient demographics, travel history, clinical presentation, diagnostic methods, and the Leishmania species involved.
Protocol and registration
The review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) guidelines [17]. Ensuring transparency, reproducibility, and methodological rigor. The protocol was prospectively registered in the PROSPERO database under ID CRD420251128116. The protocol outlines the inclusion criteria, search strategy, data extraction plan, and tools for bias assessment.
Information Sources and Search Strategy
A comprehensive literature search was performed across four databases: PubMed, Scopus, Web of Science (WoS), and Search Oxford Libraries Online (SOLO). The final search was executed on May 25, 2025. Search terms included combinations of keywords and MeSH terms related to leishmaniasis, its clinical forms (cutaneous, mucocutaneous, visceral), travel, and Europe. Boolean operators and filters were applied to refined results. An example of the PubMed search string is: (leishmaniasis [MeSH Terms] OR cutaneous leishmaniasis OR visceral leishmaniasis OR mucocutaneous leishmaniasis) AND (travel OR imported OR migration) AND (Europe).
Eligibility Criteria
Inclusion Criteria
- Case reports, case series, surveillance reports, and clinical studies providing primary data on imported human leishmaniasis diagnosed in Europe.
- Articles published between January 1, 2000, and December 31, 2024.
- Publications in English or Spanish.
- Studies reporting: patient age and sex, travel or migration history, country of exposure (imported due to infection acquired outside Europe), country of diagnosis (within Europe), clinical presentation, diagnostic method, and Leishmania species identified. For cases diagnosed in European countries with established autochthonous transmission (e.g., Spain, Italy), an infection was classified as imported strictly if the primary literature confirmed a recent travel history to a non-European endemic region coupled with the molecular or clinical identification of a non-native Leishmania species (e.g., L. braziliensis, L. panamensis, or L. major).
Exclusion Criteria
- Studies reporting only autochthonous cases within Europe.
- Veterinary cases or zoonotic surveillance without human data.
- Articles in languages other than English or Spanish.
- Studies lacking laboratory-confirmed diagnosis of leishmaniasis.
Language restrictions were based on reviewer proficiency and are acknowledged as a limitation. Laboratory confirmation was required to ensure diagnostic accuracy for epidemiological analysis.
Study Selection and Data Extraction
Two reviewers independently screened titles and abstracts using Rayyan (blind mode enabled) [18]. Full-text articles were assessed for eligibility based on the criteria above. Discrepancies were resolved by consensus. A PRISMA flow diagram illustrating the study selection process is presented in Figure 1.
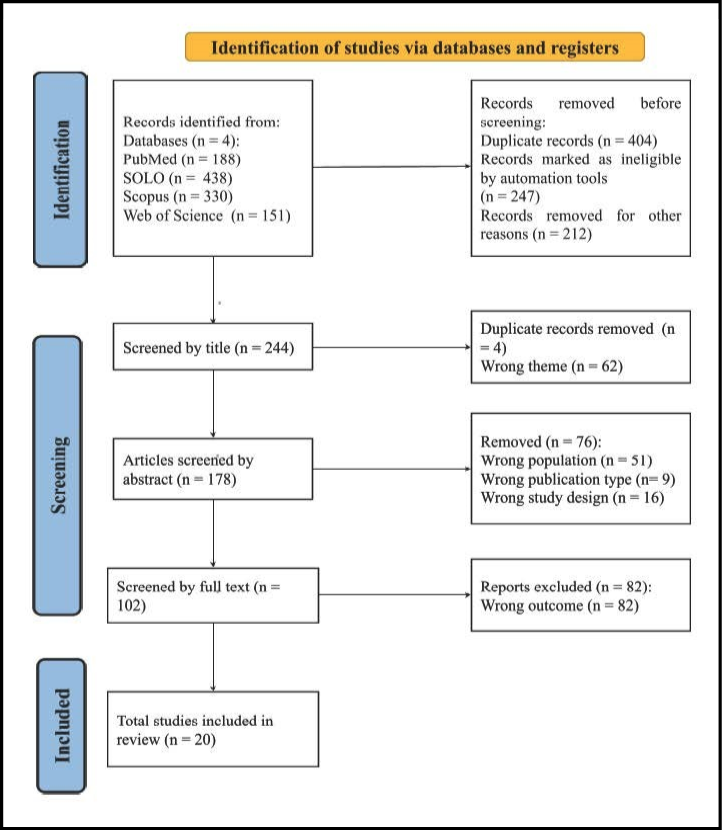
Figure 1 - PRISMA 2020 flow diagram for study selection.
Data were extracted using a standardized form developed in Microsoft Excel 365 (Version 2505. Build 18827.20176). Extracted variables included: study title, publication year, European country of diagnosis, country of exposure, number of cases, patient demographics, travel status (tourist vs. migrant), clinical form, diagnostic method, and Leishmania species. The form was piloted on five randomly selected studies to ensure consistency and completeness.
Visualizations were generated using Datawrapper with accessibility-optimized palettes.
Bias assessment
Risk of bias was assessed independently by both reviewers using the Joanna Briggs Institute (JBI) Critical Appraisal Checklists for Case Reports and Case Series. Discrepancies were resolved through consensus. Inter-rater agreement was measured using Cohen’s kappa coefficient. The JBI tools assess methodological rigor and internal validity across various domains, including patient selection, diagnostic accuracy, outcome reporting, and clinical relevance. Five case reports and seven case series met the inclusion criteria and were appraised accordingly. Detailed scoring and justification are provided in the Supplementary Material (Table S1).
Table S1 - Complete information about the studies and the extracted data.
|
n° |
Study Title |
Study ID |
Publication year |
European country of diagnosis |
Foreign country/continent of exposure |
Total number of cases |
Patient(s) sex and/or age [range] |
Type of Traveler |
Causal Leishmania species |
Clinical presentation of Leishmania |
Diagnostic method |
Treatment |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
1 |
Imported new world cutaneous leishmaniasis in a traveler from Slovakia |
https://doi.org/10.4149/bll_2015_040 |
2015 |
Slovakia |
Ecuador |
1 case |
31-year-old woman |
Tourist |
Leishmania (Viannia) panamensis |
Cutaneous leishmaniasis |
PCR |
Sodium stibogluconate at a dosage of 20 mg/kg/day for 20 days |
|
2 |
Common symptoms, rare diagnosis – pediatric visceral leishmaniasis in a non-endemic region |
https://doi.org/10.5114/polp.2024.143190 |
2024 |
Poland |
Mediterranean Sea Region (Croatia, Spain, Italy) and South America (Colombia, Brazil) |
1 case |
5-year-old girl |
Tourist |
Leishmania spp. |
Visceral leishmaniasis |
PCR |
28-day infusions of pentavalent antimonial-meglumine antimoniate, in a dose of 20 mg/kg body weight |
|
3 |
American cutaneous leishmaniasis as a rare imported disease in Europe: A case report favorably treated with antimonial derivatives |
https://doi.org/10.1023/a:1015622016579 |
2001 |
Italy |
Brazil |
1 case |
16-year-old male |
Tourist |
Leishmania (Viannia) braziliensis |
Cutaneous leishmaniasis |
Immunofluorescence serology and culture on Novy-McNeal-Nicolle medium |
Meglumine antimoniate at 20 mg/kg/day i.m. |
|
4 |
A severe case of visceral leishmaniasis and liposomal amphotericin B treatment failure in an immunosuppressed patient 15 years after exposure |
https://doi.org/10.1186/s12879-017-2192-4 |
2017 |
Switzerland |
Sudan, Bangladesh, Suriname, and Indonesia |
1 case |
80-year-old male |
Worker |
Leishmania (Leishmania) donovani complex |
Visceral |
Biopsy and PCR |
Liposomal amphotericin B with a dose of 3 mg/kg/day on days 1–5, 14, 21, and weekly thereafter |
|
5 |
Imported cutaneous leishmaniasis in a short-term traveler returning from Central Mali - The role of PCR |
https://doi.org/10.1016/j.tmaid.2012.01.004 |
2012 |
France |
Mali, West Africa |
1 case |
48-year-old male |
Tourist |
Leishmania (Leishmania) major |
Cutaneous |
A biopsy was taken from the periphery of the lesion, placed on a tissue impression smear, stained with Giemsa, and examined directly under a microscope |
IV infusions of liposomal amphotericin |
|
6 |
Successful Diagnosis and Treatment 50 Years After Exposure: Is Mucocutaneous Leishmaniasis Still a Neglected Differential Diagnosis? |
https://doi.org/10.1111/j.1708-8305.2008.00261.x |
2008 |
Germany |
Brazil |
1 case |
75-year-old male |
Worker |
Leishmania (Viannia) braziliensis |
Mucocutaneous |
Biopsy, PCR, and sequencing |
Liposomal amphotericin B (IV) 1 mg/kg bodyweight for 28 d, Miltefosine (oral) 50 mg twice daily for 28 d, and Interferon gamma (SC) 50 mcg on days 0 and 28, and 100 mcg on days 1, 2, 29, and 30 |
|
7 |
Case Report: Progressive Perforation of the Nasal Septum due to Leishmania major: A Case of Mucosal Leishmaniasis in a Traveler |
https://doi.org/10.4269/ajtmh.16-0809 |
2017 |
Austria |
South America and Spain |
1 case |
41-year-old male |
Tourist |
Leishmania (Leishmania) major |
Mucocutaneous |
Biopsy, histopathological studies, serology, PCR, and sequencing |
Liposomal amphotericin B (IV) as a cumulative dose of 30 mg/kg body weight |
|
8 |
Localized Lymphadenopathy Due to Leishmanial Infection |
https://doi.org/10.1007/s15010-001-1080-3 |
2001 |
Germany |
Spain, Guatemala, Mexico, Ecuador, and Peru |
1 case |
25-year-old female |
Tourist |
Leishmania (Leishmania) infantum |
Visceral |
Biopsy, histopathological studies, serology, and PCR |
Liposomal amphotericin B (IV) 3 mg/kg/d on days 1–5 and on day 10 |
|
9 |
Successful Treatment of Imported Mucosal Leishmania infantum Leishmaniasis With Miltefosine After Severe Hypokalemia Under Meglumine Antimoniate Treatment |
https://doi.org/10.1111/j.1708-8305.2011.00572.x |
2012 |
Switzerland |
Italy, Greece, Spain, Morocco, Egypt |
1 case |
64-year-old female |
Tourist |
Leishmania (Leishmania) infantum |
Mucocutaneous |
PCR |
Miltefosine 30-days |
|
1 |
Imported Leishmaniasis: A Heterogeneous Group of Diseases |
https://doi.org/10.1111/j.1708-8305.2009.00341.x |
2009 |
Spain |
Brazil (n=1), Algeria (n=1), Burkina Faso (n=1), Panama (n=2), Ecuador (n=1), Colombia (n=1), Costa Rica (n=2), Peru (n=1), Morocco (n=1), French Guiana (n=1) |
18 cases |
Mean age 37 years, range: 17–50 years. Male (n=12), Female (n=6) |
Immigrants (n=6) and Tourists (n=12) |
Leishmania (Viannia) braziliensis |
Cutaneous leishmaniasis (n=12), Mucocutaneous leishmaniasis (n=4), and Visceral leishmaniasis (n=2) |
Histological and Giemsa-stained smear examination, culture on Novy-McNeal-Nicolle medium, and PCR |
Pentavalent antimonials (n=14), Liposomal amphotericin B (n=8), Miltefosine (n=3), Itraconazole (n=2), ketoconazole (n=1), Pentoxifyline (n=1), allopurinol (n=1), immunotherapy (n=1) |
|
2 |
Unusual Unsatisfactory Treatment in Two Patients with Imported Cutaneous Leishmaniasis |
https://doi.org/10.3390/tropicalmed9100227 |
2024 |
Poland |
Peru (n=1), Costa Rica, and the Dominican Republic (n=1) |
2 cases |
Mean age 33 years, range: 26–40 years. Male (n=2) |
Tourists (n=2) |
Leishmania spp., Leishmania (Viannia) panamensis |
Cutaneous leishmaniasis (n=2) |
Microscopy and PCR |
Pentamidine isethionate treatment (n=1), Meglumine antimoniate (n=1) |
|
3 |
Clinical findings and management of imported cutaneous leishmaniasis: Report of 14 cases from Austria |
https://doi.org/10.1016/j.tmaid.2013.03.002 |
2013 |
Austria |
Syria (n=2), Greece (n=1), Belize (n=1), Tunisia (n=1), Spain (n=1), Unknown (n=1), Ecuador (n=1), United Arab Emirates (n=1), Bolivia (n=1), India-China (n=1), Morocco-Spain (n=1), Morocco (n=1) |
14 cases |
Mean age 25 years, range: 1–78 years. Male (n=10), Female (n=4) |
Tourists (n=14) |
Leishmania (Leishmania) donovani complex, Leishmania (Leishmania) major, Leishmania (Viannia) guyanensis complex |
Cutaneous leishmaniasis (n=14) |
Histological and PCR |
Liposomal amphotericin B (n=3), Fluconazole (n=2), cryotherapy (n=2), paromomycin (n=2), miltefosine (n=1), excision (n=1), photodynamic therapy (n=1), none (n=5) |
|
4 |
Leishmaniasis in Germany |
https://doi.org/10.3201/eid0907.030023 |
2003 |
Germany |
Belize (n=2), Bolivia (n=1), Brazil (n=3), Ecuador (n=2), French Guiana (n=2), Guatemala (n=1), Peru (n=3), Afghanistan (n=2), United Arab Emirates (n=1), Syria (n=2), Turkey (n=2), Egypt (n=2), Kenya (n=1), Libya (n=1), Angola (n=1), Tunisia (n=1), China (n=1), Iran (n=1) |
29 cases |
Mean age 31.96 years, range: 3–67 years. Male (n=20), Female (n=9) |
Tourists (n=21), Immigrants (n=4), Workers (n=4) |
Leishmania (Leishmania) donovani complex, Leishmania (Viannia) braziliensis complex, Leishmania (Leishmania) mexicana, Leishmania (Leishmania) tropica |
Mucocutaneous leishmaniasis (n=25), Visceral leishmaniasis (n=4) |
Smears, culture, histologic sections, PCR |
Liposomal amphotericin B (n=15), IFN-gamma (n=1), Systemic pentavalent antimonials (n=2), ketoconazole (n=1), Aminosidine ointment (n=5), Antibiotic (n=1), Perilesional pentavalent antimonials (n=4) |
|
5 |
Treatment of imported New World cutaneous leishmaniasis in Germany |
https://doi.org/10.1111/j.1365-4632.2011.04987.x |
2011 |
Germany |
Bolivia (n=2), Brazil (n=3), Costa Rica (n=7), Ecuador (n=4), Guyana (n=2), Peru (n=4) |
23 cases |
Mean age: 40 years, range: 17–69 years. Male (n=16), Female (n=7) |
Tourists (n=23) |
Leishmania (Viannia) braziliensis |
Cutaneous (n=23) |
PCR |
Liposomal amphotericin B (n=14), meglumine (n=5), miltefosine (n=3) |
|
6 |
Imported cutaneous leishmaniasis: a 13-year experience of a Polish tertiary center |
https://doi.org/10.5114/ada.2019.82830 |
2019 |
Poland |
Central or South America (n=7), Central or South East Asia (n=4), and Africa (n=3) |
14 cases |
Mean age: 28.5 years, range: 23–61 years. Male (n=13), Female (n=1) |
Tourists (n=10), Military (n=2), Professionals (n=2) |
Leishmania spp., Leishmania (Leishmania) major |
Cutaneous (n=14) |
Biopsy, Giemsa-stained, PCR |
Systemic pentavalent antimonials (n=7), Ketoconazole (n=3), Miltefosine (n=1), Cryotherapy (n=3) |
|
7 |
The review of imported visceral leishmaniosis in the Czech Republic |
PMID: 11396129 |
2001 |
Czech Republic |
Somalia (n=1), Croatia (n=2), Italy (n=1) |
4 cases |
Mean age 24.5 years, range: 7–45 years. Male (n=4) |
Refugee (n=1), Tourists (n=3) |
Leishmania (Leishmania) donovani |
Visceral (n=4) |
Antibody against L. donovani. Liver biopsy, indirect hemagglutination of L. donovani. Bone marrow biopsy + microscopy; indirect hemagglutination of L. donovani. Spleen puncture, microscopy, and indirect hemagglutination of L. donovani. |
Liposomal amphotericin B (n=4) |
Satistical Analysis
A series of logistic regression models was conducted to evaluate associations between traveler classification and selected demographic and clinical predictors. Initially, a multinomial logistic regression analysis (Table 1) was conducted to assess the relationship between traveler type (immigrant, refugee, tourist, expatriate, military, and worker) and age, sex, and clinical presentation (cutaneous, mucocutaneous, and visceral). To refine interpretability and address sparse-data bias, additional binary logistic models were fitted to compare tourist status against all other traveler types, using both continuous age and stratified age groups (<30, 30–50, >50). Interaction terms (e.g., sex × clinical presentation) were examined to investigate potential effect modification. Model fit was evaluated using deviance, Akaike Information Criterion (AIC), and McFadden’s pseudo-R². Fisher’s exact test was applied to assess the association between age group and traveler classification. Odds ratios (OR) with 95% confidence intervals (CI) were calculated, and a p-value <0.05 was considered statistically significant. All analyses were performed in RStudio (v4.3.1) using the broom, nnet, and openxlsx packages.
Table 1 - Complete information on 127 imported cases of leishmaniasis across Europe.
|
Study (Year) |
n |
Diagnosis Country |
Exposure Region |
Traveler Type |
Leishmania Species |
Clinical Form |
Diagnostic Method |
Core Treatment |
|---|---|---|---|---|---|---|---|---|
|
Alcocer-Veintimilla (2015) |
1 |
Slovakia |
Ecuador |
Tourist |
Leishmania (Viannia) panamensis |
CL |
PCR |
Sodium stibogluconate |
|
Pediatric VL |
1 |
Poland |
Mediterranean, S. America |
Tourist |
Leishmania spp. |
VL |
PCR |
Meglumine antimoniate |
|
American CL (2001) |
1 |
Italy |
Brazil |
Tourist |
Leishmania (Viannia) braziliensis |
CL |
Serology, Culture |
Meglumine antimoniate |
|
Severe VL |
1 |
Switzerland |
Sudan, Bangladesh, Suriname, Indonesia |
Worker |
Leishmania (Leishmania) donovani complex |
VL |
Biopsy, PCR |
Liposomal amphotericin B (L-AmB) |
|
Imported CL |
1 |
France |
Mali |
Tourist |
Leishmania (Leishmania) |
CL |
Microscopy |
L-AmB |
|
ML 50yr |
1 |
Germany |
Brazil |
Worker |
Leishmania (Viannia) braziliensis |
ML |
Biopsy, PCR, Sequencing |
L-AmB, Miltefosine, IFN-gamma |
|
Mucosal Leishmaniasis (2017) |
1 |
Austria |
S. America, Spain |
Tourist |
Leishmania (Leishmania) |
ML |
Biopsy, Histology, Serology, PCR, Sequencing |
L-AmB |
|
Localized Lymphadenopathy (2001) |
1 |
Germany |
Spain, Guatemala, Mexico, Ecuador, Peru |
Tourist |
Leishmania (Leishmania) infantum |
VL |
Biopsy, Histology, Serology, PCR |
L-AmB |
|
Mucosal |
1 |
Switzerland |
Italy, Greece, Spain, Morocco, Egypt |
Tourist |
Leishmania (Leishmania) infantum |
ML |
PCR |
Miltefosine |
|
Alcocer-Veintimilla (2009) |
18 |
Spain |
Americas, Africa |
Immigrants, Tourists |
Leishmania (Viannia) braziliensis |
CL, ML, VL |
Histology, Culture, PCR |
Antimonials, L-AmB, Miltefosine, Others |
|
Unusual Treatment (2024) |
2 |
Poland |
Peru, Costa Rica, Dominican Rep. |
Tourists |
Leishmania spp., |
CL |
Microscopy, PCR |
Pentamidine isethionate, Meglumine antimoniate |
|
Austria Series (2013) |
14 |
Austria |
Global |
Tourists |
L. (L.) donovani complex, |
CL |
Histology, PCR |
L-AmB, Fluconazole, Paromomycin, Miltefosine, Others |
|
Germany Series (2003) |
29 |
Germany |
Global (Mixed) |
Tourists, Immigrants, Workers |
L. (L.) donovani complex, |
ML, |
Smears, Culture, Histology, PCR |
L-AmB, IFN-gamma, Antimonials, Aminosidine |
|
Treatment New World CL |
23 |
Germany |
Americas |
Tourists |
Leishmania (Viannia) braziliensis |
CL |
PCR |
L-AmB, Meglumine antimoniate, Miltefosine |
|
Polish Center (2019) |
14 |
Poland |
Americas, Asia, Africa |
Tourists, Military, Professionals |
Leishmania spp., |
CL |
Biopsy, Giemsa, PCR |
Antimonials, Ketoconazole, Miltefosine, Cryotherapy |
|
Czech Republic Series |
4 |
Czech Republic |
Somalia, Croatia, Italy |
Refugee, Tourists |
Leishmania (Leishmania) donovani |
VL |
Antibody, Biopsy, Microscopy |
L-AmB |
Note: Detailed patient demographics, exact treatment dosages, and full study identifiers are available in the Supplementary Material (Table S1).
Deviations from the original Protocol
No significant changes or deviations from the initial protocol described have been made.
RESULTS
Study Selection and Screening
The screening process was conducted using Rayyan systematic review software, as illustrated in Figure 1. Of the four databases searched, three yielded relevant results, generating a total of 1,107 articles. After removing 863 records due to duplication and exclusion based on population (e.g., veterinary cases), publication type (e.g., editorials), and study design (e.g., narrative reviews), 102 articles were retained for full-text screening. Following further eligibility assessment, 82 articles were excluded, leaving 20 studies for final inclusion. Data extraction matrices are provided in the Supplementary Material (Table S1).
Epidemiological Overview of Imported Cases
A total of 127 published cases of imported leishmaniasis were extracted from the included literature across Europe (Table 2). The distribution of cases by country is shown in Figure 2. Germany reported the highest number of cases (n=58; 46%), followed by Spain (n=19; 15%), Poland (n=17; 13%), Austria (n=15; 12%), France (n=6; 5%), Czech Republic (n=4; 3%), Switzerland (n=3; 2%), Netherlands (n=2; 2%), and Italy, England, and Slovakia with one case each (1%).
Table 2 - Binary Logistic Regression.
|
Predictor |
OR |
Std error |
statistic |
P value |
CI Lower |
CI Upper |
|
(Intercept) |
6,614 |
0,662 |
2,854 |
0,004 |
1,904 |
26,054 |
|
Age |
0,994 |
0,013 |
-0,475 |
0,635 |
0,969 |
1,02 |
|
Sex Male |
0,856 |
0,5 |
-0,311 |
0,756 |
0,303 |
2,212 |
|
Clinical Presentation Mucocutaneous |
0,581 |
0,489 |
-1,11 |
0,267 |
0,224 |
1,554 |
|
Clinical Presentation Visceral |
0,243 |
0,639 |
-2,217 |
0,027 |
0,068 |
0,868 |
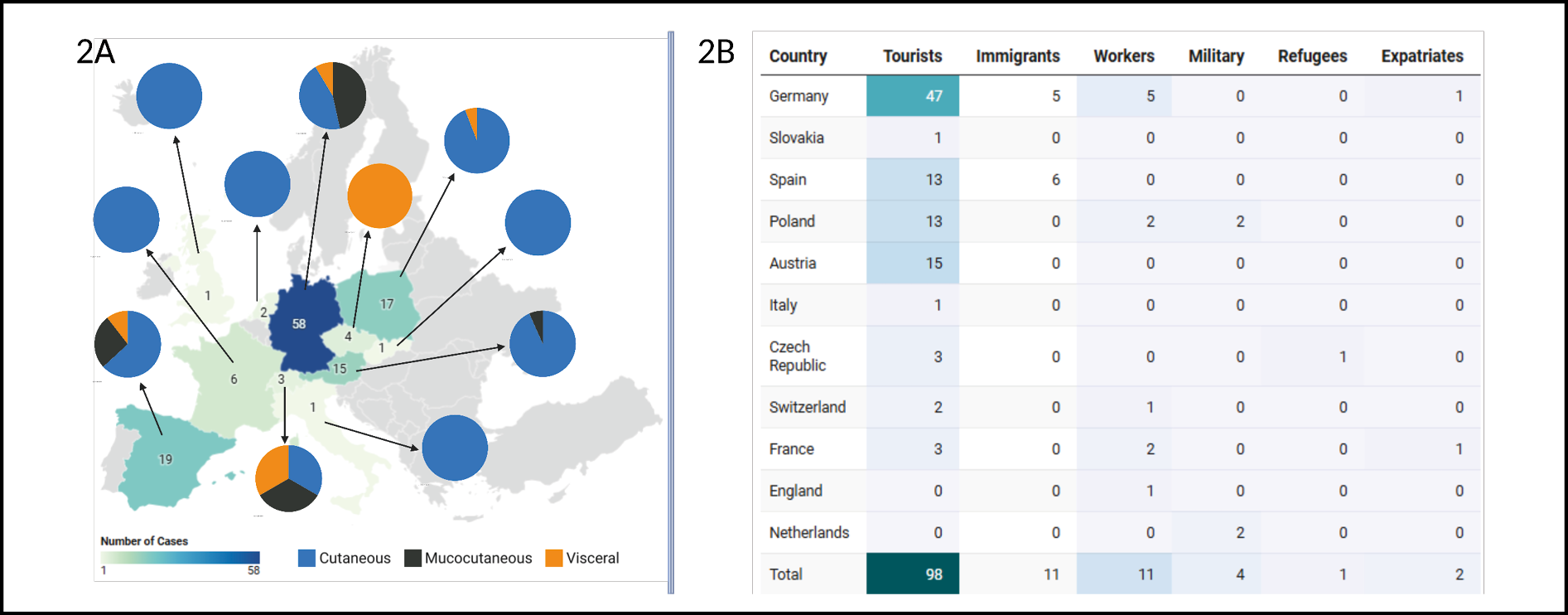
Figure 2 - Imported Leishmaniasis cases in Europe, 2000–2024.
2A - Geographic distribution of reported cases by country of importation, with overlaid pie charts showing the proportion of clinical presentations (cutaneous, mucocutaneous, and visceral) for each country. In countries with endemic transmission (e.g., Spain, Italy), imported status was verified by identifying non-native species and travel exposure outside Europe.
2B - Number of reported cases by country of importation and traveler type (tourists, immigrants, workers, military personnel, refugees, and expatriates).
Clinical Presentation and Traveler Typology
Among the 127 cases, cutaneous leishmaniasis (CL) was the most frequently reported clinical form (n=80; 63%), followed by mucocutaneous leishmaniasis (ML) (n=34; 27%) and visceral leishmaniasis (VL) (n=13; 10%). Data regarding underlying comorbidities and immune status were inconsistently reported across the included studies; however, at least one case of severe visceral leishmaniasis was explicitly documented in an immunosuppressed patient experiencing treatment failure. Germany reported all three clinical forms, with CL (n=26), ML (n=27), and VL (n=5) (Figure 2). Poland showed a predominance of CL (n = 16), while VL was most notable in the Czech Republic (n = 4) and Germany. ML was more localized, with cases concentrated in Germany, Spain, and Austria.
Traveler classification revealed that tourists accounted for the majority of cases (n=98; 77%), followed by immigrants (n=11; 9%), workers (n=11; 9%), military personnel (n=4; 3%), expatriates (n=2; 2%), and refugees (n=1; 1%). Country-specific breakdowns are shown in Figure 2. Germany had the highest number of tourists (n = 47), immigrants (n = 5), and workers (n = 5), as well as one expatriate. Spain reported tourists (n = 13) and immigrants (n = 6), while Poland included tourists (n = 13), workers (n = 2), and military personnel (n = 2). Other countries primarily reported tourists, with minimal representation from other traveler categories.
Exposure Geography
The global distribution of exposure countries is presented in Figure 3. Peru was the most frequently visited country (n = 11), followed by Costa Rica, Brazil, Ecuador (n = 10 each), Bolivia (n = 8), and Mexico (n = 7). The remaining countries reported fewer than 5 exposures. Detailed exposure data, categorized by country of diagnosis and travel destination, are provided in Table 1.
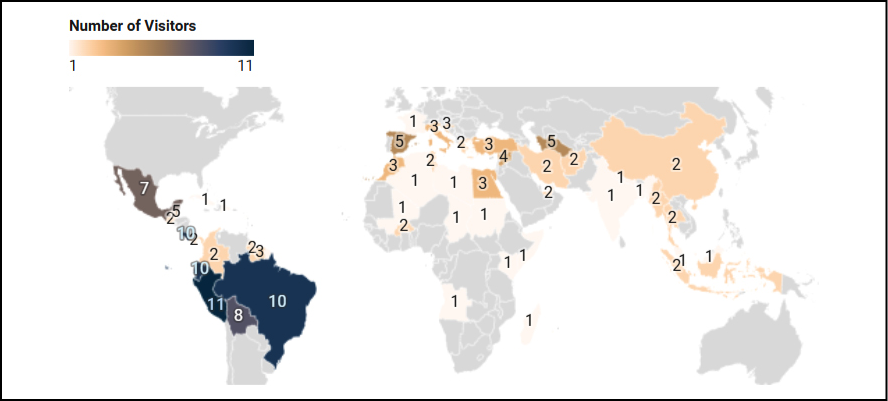
Figure 3 - Potential countries of exposure for imported cases of Leishmaniasis in Europe, 2000-2024.
Note (1): Geographic distribution of potential exposure countries visited by individuals later diagnosed with imported Leishmaniasis in Europe. Only destinations where Leishmania spp. are known to be endemic are shown. The color gradient represents the number of visitors per country.
Note (2): As some travelers visited more than one endemic country, these are classified as “potential” exposure sites.
Diagnostic methods and species identification
All cases included in this review were laboratory-confirmed, using one or more of the following diagnostic methods:
- Polymerase Chain Reaction (PCR)
- Histological examination
- Giemsa-stained smears
- Novy-McNeal-Nicolle (NNN) culture
- Immunofluorescence serology
- Biopsy
The most frequently employed techniques were PCR, histology, and Giemsa staining, reflecting current diagnostic standards for leishmaniasis.
- Species identification revealed a diverse range of Leishmania spp., including:
- Leishmania (Viannia) panamensis
- L. braziliensis
- L. panamensis
- L. donovani/infantum complex
- L. major
- L. guyanensis complex
- Leishmania (Viannia) braziliensis
- L. mexicana
- L. tropica
- Leishmania spp. (unspecified)
Species identification was closely linked to the diagnostic method used and the geographic origin of exposure.
Treatment modalities
Most patients were treated with either:
Treatment regimens were highly heterogeneous, reflecting the diverse clinical presentations and national protocols across the reporting centers. For cutaneous leishmaniasis, the most common regimen was systemic pentavalent antimonials at 20 mg/kg/day for 20 to 28 days. Visceral leishmaniasis was primarily managed with liposomal amphotericin B, at doses ranging from 3 mg/kg/day to a cumulative dose of 30 mg/kg. Reported outcomes were generally favorable, with the majority of studies documenting clinical cure; however, treatment failure and relapse were observed, particularly in immunosuppressed patients. Data on follow-up duration were inconsistently reported, limiting our ability to establish definitive long-term cure rates. Detailed treatment data are available in the Supplementary Material (Table S1).
Regression results: profiles in imported leishmaniasis
Regression analysis showed that visceral leishmaniasis was significantly less common among tourists than among other traveler types (OR: 0.24; 95% CI: 0.07–0.87; p = 0.027), while age and sex did not have predictive value in any of the models. Age-stratified comparisons (<30, 30–50, >50 years) confirmed no demographic associations, and Fisher’s exact test found no significant relationship between age group and traveler classification (p = 0.92). Interaction analysis between sex and clinical presentation did not reveal any effect modification. The multinomial logistic regression yielded inflated odds ratios due to sparse-category bias and quasi-complete separation, thereby limiting interpretability. Across all models, clinical presentation, especially visceral form, was the only variable consistently associated with traveler classification. For complete statistical outputs and model diagnostics, see Table S1.
DISCUSSION
Our findings confirm the predominance of cutaneous leishmaniasis (CL) in imported cases, consistent with Eurosurveillance data [19]. However, the proportion of visceral leishmaniasis (VL) was lower in our cohort compared to their report. The incidence of imported leishmaniasis in Europe has fluctuated, with periods of increase and decrease. WHO data show fluctuating trends in imported cases of CL and VL across Europe, with a notable decline from 2013 to 2023 [10]. One study reviewing the prevalence of cutaneous leishmaniasis in Europe from 2013 to 2019 highlights transmission of L. tropica and L. major among travelers, especially immigrants [20]. These patterns underscore the need for consistent surveillance and may reflect changes in travel behavior or diagnostic capacity [11]. Moreover, based on our findings, the patient types infected with Leishmania align with the Eurosurveillance report, which shows that tourists are most affected (27.1%), followed by immigrants (17.1%) [19]. Although tourists and male patients were the most frequently affected groups, our regression models found no significant association between traveler classification and age or sex, suggesting that behavioral exposure may outweigh demographic risk factors [19].
According to the European Center for Disease Prevention and Control (ECDC), leishmaniasis emerging in non-endemic areas is closely associated with international travel, which facilitates the introduction of non-endemic species alongside local strains [21]. The co-circulation of these diverse lineages creates conditions that are ripe for the emergence of hybrid parasites [22]. As recently highlighted in the literature, hybridization at this genetic crossroads can fundamentally reshape disease patterns by altering transmission dynamics, enhancing vector adaptability to new ecological niches, and potentially modifying clinical virulence or drug susceptibility profiles [22].
This complex genetic mixing raises significant public health concerns, particularly regarding the risk of onward transmission in naive populations or among immunocompromised individuals, who may act as prolonged reservoirs for these novel hybrid strains [10, 22]. Tourists account for most reported cases, highlighting changing patterns of travel exposure. Adventure travel, ecotourism, and occupational trips often take place in rural or wilderness areas, where there is a higher risk of exposure to sandflies. Ecotourism’s rise has increased the number of imported cases in Europe [6]. Ecotourism and occupational deployments increasingly place travelers in vector-endemic environments, elevating the risk of sandfly exposure and potential introduction of non-native Leishmania species into Europe [5, 6, 13].
Environmental factors significantly influence the spread of leishmaniasis in non-endemic areas, with global warming being a key factor. Climate change impacts sandfly populations, affecting disease cases by altering conditions that determine sandflies’ survival, reproduction, distribution, and activity [15]. Some of these factors include rising temperatures, as sandflies thrive in warm climates, with optimal activity and reproduction [23]. As temperatures rise, more regions become suitable for sandflies, increasing their population and range. Models suggest moderate climate change could create habitats in Central Europe, especially in temperate and mild winter areas, but they are already established near the Mediterranean coast [14]. A study found that under strong climatic forcing, CL is more sensitive to extreme climate change, leading to a reduction in its distribution, but this does not mean it will be eradicated [24].
Early detection is crucial in preventing severe outcomes and limiting leishmaniasis morbidity. Polymerase chain reaction (PCR) is the most utilized diagnostic method, offering high sensitivity. This high sensitivity is particularly relevant given the diagnostic variability and frequent underestimation of human visceral leishmaniasis prevalence observed when comparing molecular methods to traditional serology and microscopy in highly endemic regions such as Latin America [25]. Microscopic observation of amastigotes, although the traditional gold standard, is less sensitive but faster, taking about an hour, while PCR takes around six hours, making it more suitable for second and third-level healthcare facilities [12]. Additionally, PCR enables the molecular characterization of Leishmania species, providing a broader epidemiological perspective on leishmaniasis cases [26]. Crucially, from a clinical standpoint, species-specific identification via PCR directly informs the prognosis and therapeutic approach by alerting clinicians to species associated with potentially complicated clinical forms, such as the well-established risk of mucocutaneous leishmaniasis (ML) following L. braziliensis infection [26]. Furthermore, loop-mediated isothermal amplification (LAMP) can be used as a point-of-care testing method in resource-limited settings with endemic diseases, serving as an alternative diagnostic approach [27]. In Europe, institutions like the ECDC offer these tools or make them available across various countries; however, diagnosis is challenging in countries where the disease is not endemic, and medical staff may lack familiarity with its presentation and management [6]. A delayed diagnosis can lead to increased transmission, complications, and strain on healthcare services. Local response manages imported leishmaniasis, but prevention is vital to prevent a global health crisis. Globally, promoting pre-travel advice is crucial for raising awareness of Leishmania prevention among travelers.
In accordance with the current Infectious Diseases Society of America (IDSA) and American Society of Tropical Medicine and Hygiene (ASTMH) guidelines, the management of leishmaniasis is tailored to the clinical syndrome and infecting species [28]. For complex cutaneous leishmaniasis (CL), systemic pentavalent antimonials, such as sodium stibogluconate (SSG) and meglumine antimoniate (MA), are established treatments dosed at 20 mg/kg/day for 20 to 28 days [28, 29]. For uncomplicated or localized CL, IDSA guidelines strongly recommend local therapies, such as intralesional antimonials combined with cryotherapy or thermotherapy, to improve cure rates while minimizing systemic toxicity [28, 30]. Additionally, topical paromomycin and oral miltefosine are alternative options, while liposomal amphotericin B is often used for refractory cases [28, 31]. Mucocutaneous leishmaniasis (ML) poses significant therapeutic challenges; however, systemic antimonials or liposomal amphotericin B are recommended, with the latter demonstrating up to 90% efficacy and a favorable safety profile [28, 32]. Furthermore, the IDSA guidelines designate liposomal amphotericin B as the Food and Drug Administration (FDA) approved drug of choice for visceral leishmaniasis (VL) in Europe and the Americas due to its high efficacy and shorter treatment course [28, 33] to its high efficacy, shorter treatment course, and its favorable safety profile [33, 34].
However, in Eastern Africa, combination therapy with sodium stibogluconate and paromomycin remains the standard of care, with randomized controlled trials confirming its efficacy and safety (29). More recently, oral miltefosine combined with injectable paromomycin has demonstrated cure rates exceeding 90%, offering a shorter, less invasive, and more accessible alternative [35, 36]. Parenteral paromomycin, however, is not readily available in Europe, which complicates treatment options outside endemic regions.
Regarding clinical response, our review highlights that outcomes for imported leishmaniasis are generally comparable to those documented for indigenous European cases, if diagnosis and treatment initiation are timely. However, imported cases often face a higher risk of diagnostic delay, a factor that may complicate therapeutic management, compared with indigenous cases, where clinical suspicion is higher due to endemicity. Furthermore, the therapeutic response in imported cases is significantly influenced by the infecting species and potential prior exposures, underscoring that while the clinical course mirrors indigenous forms, the path to diagnosis and treatment is often uniquely challenging for the traveler population
Importantly, therapeutic decisions must consider regional guidelines, drug availability, patient comorbidities, and resistance patterns. Particular attention is warranted for HIV coinfected and other immunosuppressed patients, in whom treatment outcomes are more difficult to achieve and relapse rates are higher [34]. Visceral leishmaniasis in immunocompromised hosts presents distinct diagnostic and therapeutic challenges, necessitating tailored clinical approaches and careful evaluation of established guidelines to prevent complications and clinical failure [37]. These challenges underscore the need for individualized, context-specific strategies to ensure both efficacy and safety.
This review systematically analyzed factors associated with imported Leishmania cases in Europe. A strength was the inclusion of a consistent set of cases, which provided uniform clinical, epidemiological, and travel data, enabling reliable comparisons. However, many studies were excluded due to incomplete information, limited access, or language barriers, making standardization difficult. Despite these issues, the review provided valuable insights into surveillance, diagnosis, and risk assessment in non-endemic regions.
The regression analyses reveal the complexity of modeling traveler classification in imported leishmaniasis, given the limited cases reported in this study. Visceral presentation was less common among tourists, and neither age nor sex was a strong predictor, which challenges typical travel medicine assumptions. The lack of association with age suggests that exposure risk is more behaviorally driven than demographically. The multinomial model, although ambitious, encountered issues such as quasi-complete separation and bias from sparse categories, leading to high odds ratios. This highlights the limitations of applying high-dimensional models to small sample sizes. Using penalized regression or collapsing categories could enhance stability. The absence of interaction effects between sex and clinical form indicates that disease presentation is similar across genders among travelers in our findings, aligning with broader data but requiring cautious interpretation due to the sample structure.
From a public health perspective, the prevalence of cutaneous leishmaniasis among tourists highlights the importance of targeted pre-travel counseling, particularly for those engaging in ecotourism and adventure travel. While PCR is a highly effective diagnostic tool, its limited availability remains a challenge primarily in endemic, resource-constrained settings; in Europe, PCR is generally accessible, and underdiagnosis is more plausibly attributable to limited clinical awareness or underreporting rather than lack of diagnostic capacity [6]. These findings reinforce the need for enhanced surveillance systems that integrate travel history, clinical presentation, and diagnostic methods. Future research should prioritize prospective data collection, standardized case definitions, and species- and location-specific analyses to better characterize risks and inform effective prevention strategies.
LIMITATIONS
This review is subject to several limitations that affect the generalizability and depth of its findings. First, reliance on published case reports and series introduces selection and publication bias, tending to overrepresent severe or atypical presentations while underreporting mild or asymptomatic cases, which are relatively common but seldom documented. This imbalance highlights the need for more systematic data collection to capture the full clinical spectrum of disease and improve representativeness in future analyses. Language restrictions to English and Spanish may have excluded relevant data from endemic regions in Europe, and limited access to full-text articles further constrained inclusion. The heterogeneity in diagnostic methods, species identification, and treatment reporting across studies hindered comparative analysis and precluded meta-analytic synthesis. Additionally, the classification of cases as imported versus autochthonous was inconsistently defined, often relying solely on patient-reported travel history without molecular confirmation, thereby potentially obscuring local transmission dynamics. The statistical model applied had limited power due to the sample size. Although descriptive trends were observed, no significant associations were found between age or sex and the clinical form of the disease. Climate-related insights were derived from secondary literature without integrating geospatial or environmental data, limiting the precision of ecological interpretations. Finally, treatment data were inconsistently reported and lacked standardized outcome measures, making it challenging to assess therapeutic efficacy across clinical forms and regions. These limitations underscore the need for standardized reporting, multilingual surveillance, and prospective multicenter studies to strengthen the evidence base for imported leishmaniasis in Europe.
CONCLUSIONS
This systematic review identified 127 confirmed cases of imported leishmaniasis in Europe between 2000 and 2024, with Germany, Spain, and Poland reporting the highest numbers. Most cases are imported from Latin American countries, especially Costa Rica, Peru, and Brazil. The epidemiological characteristics analyzed revealed that most imported cases were associated with male ecotourists, predominantly those aged approximately 33. Other types of travelers with other purposes, such as immigrants and workers, also stood out. Regarding the recognized Leishmania species, the majority were reported as L. braziliensis and L. panamensis (New World species), with most diagnoses made by PCR, which was among the most commonly used methods. Thus, coincidentally, the most common clinical presentation of Leishmania was cutaneous leishmaniasis.
These findings highlighted the importance of including leishmaniasis in the differential diagnosis of returning travelers with skin lesions or systemic symptoms [29]. Pre-travel counseling, including strategies to avoid vector-borne diseases, is of utmost importance. This is essential, especially for those practicing ecotourism. There was also a call to strengthen public health surveillance, diagnostic capacity, and training of health professionals in non-endemic countries to improve detection and reduce the disease burden [29].
This review presents new insights into travel medicine and infectious disease epidemiology by consolidating case-level data spanning 24 years. In addition, it supports the need to standardize the reporting of travel-related infections and to enhance this type of study by including clinical treatment and follow-up of travelers to analyze disease evolution. Ultimately, the successful management of imported leishmaniasis hinges on a diagnostic paradigm shift: viewing travel-associated skin and systemic lesions not as rare dermatological curiosities, but as primary indicators for rapid, species-specific molecular testing. By integrating systematic risk-stratification into primary care and lowering the threshold for diagnostic referral, healthcare systems can transition from reactive, late-stage management to a proactive approach that ensures timely treatment and prevents further transmission.
Funding
This review did not receive funding.
Conflict of interest
JDAE received a Travel Grant from ESGITM for that presentation.
Ai writing declaration
To write this review, we used Grammarly software to verify the accuracy of English under the strict supervision of the senior authors.
Acknowledgments
We are grateful to the Universidad Internacional Sek del Ecuador for supporting researchers by allocating research hours through the Direction of Research. This article has been registered in the Research Proposal Registration of the Coordination of Scientific Integrity and Surveillance of Universidad Cientifica del Sur, Lima, Peru, under the number PI-50-2026-1184. This article is part of a project of the European Society for Clinical Microbiology and Infectious Diseases (ESCMID) Study Group for Infections in Travellers and Migrants (ESGITM) by JDAE, AA, MGZ, and AJRM. Finally, this study was presented in part at the ESCMID Global 2026, the 36th Congress of the European Society of Clinical Microbiology and Infectious Diseases (ESCMID), as an Oral Presentation (O0941) (Session Navigating clinical realities in travelers and migrant populations - OS130), Munich, Germany, April 17-21, 2026.
Authors contribution
Sandra M. Alcocer-Veintimilla and Víctor A. Pillajo-Gangotena contributed equally to the conception of the original idea and the design of the systematic review. They carried out the execution of the review process, including data collection, analysis, and visualization, and prepared the initial draft of the manuscript. Jaime David Acosta-España, as the senior and most experienced author, supervised the entire project, coordinated the development of the manuscript, acted as the third reviewer to ensure methodological rigor, and provided strategic oversight and guidance throughout all stages of the work. Aula Abbara, Marta González-Sanz, and Alfonso J. Rodriguez-Morales, recognized experts with extensive experience in infectious diseases and global health, contributed to the in-depth analysis and interpretation of the data, contextualized the findings within the broader scientific literature, and critically revised the manuscript. Their senior expertise ensured that the study was framed within an international perspective and met the highest academic standards. All authors reviewed, approved, and agreed to the final version of the manuscript.
REFERENCES
[1] de Vries HJC, Schallig HD. Cutaneous Leishmaniasis: A 2022 Updated Narrative Review into Diagnosis and Management Developments. Am J Clin Dermatol 2022; 23: 823-840. https://doi.org/10.1007/s40257-022-00726-8.
[2] Mann S, Frasca K, Scherrer S, et al. A Review of Leishmaniasis: Current Knowledge and Future Directions. Curr Trop Med Rep. 2021; 8: 121-132. https://doi.org/10.1007/s40475-021-00232-7.
[3] Mathison BA, Bradley BT. Review of the Clinical Presentation, Pathology, Diagnosis, and Treatment of Leishmaniasis. Lab Med 2023; 54: 363-371. https://doi.org/10.1093/labmed/lmac134.
[4] Abadías-Granado I, Diago A, Cerro PA, et al. Leishmaniasis cutánea y mucocutánea. Actas Dermosifiliogr 2021; 112: 601-618. https://doi.org/10.1016/j.ad.2021.02.008.
[5] Mansueto P, Seidita A, Vitale G, et al. Leishmaniasis in travelers: A literature review. Travel Med Infect Dis 2014; 12: 563-581. https://doi.org/10.1016/j.tmaid.2014.09.007.
[6] Pavli A, Maltezou HC. Leishmaniasis, an emerging infection in travelers. Int J Infect Dis. 2010; 14: e1032–1039. https://doi.org/10.1016/j.ijid.2010.06.019.
[7] World Health Organization (WHO). Leishmaniasis: Key facts. 2023. https://www.who.int/news-room/fact-sheets/detail/leishmaniasis (accessed July 5, 2025).
[8] Centers for Disease Control and Prevention (CDC). Understanding Your Risk for Leishmaniasis 2024. https://www.cdc.gov/leishmaniasis/risk-factors/index.html (accessed August 3, 2025).
[9] World Health Organization (WHO). Global leishmaniasis surveillance updates 2024: consolidating gains and new initiatives 2025. https://www.who.int/publications/i/item/who-wer10045-535-552 (accessed December 10, 2025).
[10] Pan American Health Organization. Epidemiological Report of the Americas. Leishmaniases 2017. https://iris.paho.org/handle/10665.2/34112 (accessed April 25, 2025).
[11] World Health Organization (WHO). Leishmaniasis 2024. https://apps.who.int/neglected_diseases/ntddata/leishmaniasis/leishmaniasis.html (accessed August 16, 2025).
[12] Chicharro C, Nieto J, Miguelañez S, et al. Molecular Diagnosis of Leishmaniasis in Spain: Development and Validation of Ready-To-Use Gel-Form Nested and Real-Time PCRs To Detect Leishmania spp. Microbiol Spectr. 2023; 11(3): e0335422. https://doi.org/10.1128/SPECTRUM.03354-22.
[13] Rawat SK. A study on impact of ecotourism on wildlife: Scenario of Sariska National Park. Int J Fauna Biol Stud. 2022; 9(3): 24-28.
[14] Fischer D, Moeller P, Thomas SM, et al. Combining Climatic Projections and Dispersal Ability: A Method for Estimating the Responses of Sandfly Vector Species to Climate Change. PLoS Negl Trop Dis 2011; 5: e1407. https://doi.org/10.1371/journal.pntd.0001407.
[15] Trájer AJ, Grmasha RA. The potential effects of climate change on the climatic suitability patterns of the Western Asian vectors and parasites of cutaneous leishmaniasis in the mid- and late twenty-first century. Theor Appl Climatol 2024; 155: 1897-1914. https://doi.org/10.1007/s00704-023-04726-4.
[16] Barth-Jaeggi T, Mäser P. Leishmaniasis in Europe and Central Asia: Epidemiology, Impact of Habitat and Lifestyle Changes, HIV Coinfection. In: Steinmann P, Utzinger J, eds. Neglected Tropical Diseases - Europe and Central Asia. Springer, Cham; 2021:83 99.
[17] Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021; 372: n71. https://doi.org/10.1136/bmj.n71.
[18] Elmagarmid A, Fedorowicz Z, Hammady H, et al. Rayyan: a systematic reviews web app for exploring and filtering searches for eligible studies for Cochrane Reviews. Cochrane Colloq Abstr. 2014.
[19] Van der Auwera G, Davidsson L, Buffet P, et al. Surveillance of leishmaniasis cases from 15 European centres, 2014 to 2019: a retrospective analysis. Euro Surveill. 2022; 27(4): 2002028. https://doi.org/10.2807/1560-7917.ES.2022.27.4.2002028.
[20] Glans H, Dotevall L, Van der Auwera G, et al. Treatment outcome of imported cutaneous leishmaniasis among travelers and migrants infected with Leishmania major and Leishmania tropica: a retrospective study in European centers 2013 to 2019. Int J Infect Dis. 2022; 122: 375–381. https://doi.org/10.1016/j.ijid.2022.06.025.
[21] El-Sayed A, Kamel M. Climatic changes and their role in emergence and re emergence of diseases. Environ Sci Pollut Res Int 2020; 27: 22336. https://doi.org/10.1007/S11356-020-08896-W.
[22] Ferreira TR. At the genetic crossroads of Leishmania: Emerging hybrids reshaping disease patterns. PLoS Pathog 2025; 21: e1013213. https://doi.org/10.1371/journal.ppat.1013213.
[23] El-Sayed A, Kamel M. Climatic changes and their role in emergence and re emergence of diseases. Environ Sci Pollut Res Int. 2020; 27(18): 22336-22352. https://doi.org/10.1007/s11356-020-08896-w.
[24] Purse B V., Masante D, Golding N, et al. How will climate change pathways and mitigation options alter incidence of vector-borne diseases? A framework for leishmaniasis in South and Meso-America. PLoS One 2017; 12: e0183583. https://doi.org/10.1371/journal.pone.0183583.
[25] Gutiérrez-Ocampo E, Villamizar-Peña R, Cortes-Bonilla I, et al. Human visceral leishmaniasis prevalence by different diagnostic methods in Latin America: a systematic review and meta-analysis. Infez Med 2021; 29: 199-208.
[26] Silgado A, Armas M, Sánchez-Montalvá A, et al. Changes in the microbiological diagnosis and epidemiology of cutaneous leishmaniasis in real-time PCR era: A six-year experience in a referral center in Barcelona. PLoS Negl Trop Dis. 2021; 15: e0009884. https://doi.org/10.1371/journal.pntd.0009884.
[27] Nzelu CO, Kato H, Peters NC. Loop-mediated isothermal amplification (LAMP): An advanced molecular point-of-care technique for the detection of Leishmania infection. PLoS Negl Trop Dis. 2019; 13: e0007698. https://doi.org/10.1371/journal.pntd.0007698.
[28] Aronson N, Herwaldt BL, Libman M, et al. Diagnosis and Treatment of Leishmaniasis: Clinical Practice Guidelines by the Infectious Diseases Society of America (IDSA) and the American Society of Tropical Medicine and Hygiene (ASTMH). Clin Infect Dis. 2016; 63: E202-64. https://doi.org/10.1093/CID/CIW670.
[29] Garza-Tovar TF, Sacriste-Hernández MI, Juárez-Durán ER, et al. An overview of the treatment of cutaneous leishmaniasis. Fac Rev 2020; 9: 28. https://doi.org/10.12703/R/928.
[30] Heras-Mosteiro J, Monge-Maillo B, Pinart M, et al. Interventions for Old World cutaneous leishmaniasis. Cochrane Database Syst Rev. 2017; 11(11): CD005067. https://doi.org/10.1002/14651858.CD005067.PUB4.
[31] Chakravarty J, Sundar S. Current and emerging medications for the treatment of leishmaniasis. Expert Opin Pharmacother 2019; 20: 1251-1265. https://doi.org/10.1080/14656566.2019.1609940.
[32] Fischer T, Fischer M, Schliemann S, et al. Treatment of mucocutaneous leishmaniasis - A systematic review. J Dtsch Dermatol Ges 2024; 22: 763-773. https://doi.org/10.1111/DDG.15424.
[33] Kumari S, Kumar V, Tiwari RK, et al. Amphotericin B: A drug of choice for Visceral Leishmaniasis. Acta Trop 2022; 235: 106661. https://doi.org/10.1016/J.ACTATROPICA.2022.106661.
[34] Srivarasat S, Brownell N, Siriyasatien P, et al. Case Report: Autochthonous Disseminated Cutaneous, Mucocutaneous, and Visceral Leishmaniasis Caused by Leishmania martiniquensis in a Patient with HIV/AIDS from Northern Thailand and Literature Review. Am J Trop Med Hyg. 2022; 107: 1196-1202. https://doi.org/10.4269/AJTMH.22-0108.
[35] Musa A, Khalil E, Hailu A, et al. Sodium Stibogluconate (SSG) & Paromomycin Combination Compared to SSG for Visceral Leishmaniasis in East Africa: A Randomised Controlled Trial. PLoS Negl Trop Dis. 2012; 6: e1674. https://doi.org/10.1371/JOURNAL.PNTD.0001674.
[36] Musa AM, Mbui J, Mohammed R, et al. Paromomycin and Miltefosine Combination as an Alternative to Treat Patients With Visceral Leishmaniasis in Eastern Africa: A Randomized, Controlled, Multicountry Trial. Clin Infect Dis. 2023; 76: E1177–1185. https://doi.org/10.1093/CID/CIAC643.
[37] Pagliano P, Esposito S. Visceral leishmaniosis in immunocompromised host: an update and literature review. J Chemother. 2017; 29(5): 261-266. https://doi.org/10.1080/1120009X.2017.1323150.