Le Infezioni in Medicina, n. 2, 239-246, 2026
doi: 10.53854/liim-3402-14
INFECTIONS IN THE HISTORY OF MEDICINE
Asian Flu in Milan, 1957. A brief history of the first pandemic occurred after the discovery of Influenza A virus and its impact in a large Italian city
Massimo Galli1, Fulvio Adorni2
1Department of Biomedical and Clinical Sciences, Università degli Studi di Milano, Milan, Italy;
2Institute of Biomedical Technologies, National Research Council, Segrate, Milan, Italy.
Article received 9 February 2026 and accepted 14 April 2026
Corresponding author
Massimo Galli
E-mail: massimo.galli@unimi.it
SUMMARY
Asian flu emerged in southern China in the last months of 1956 and after reaching Singapore and Hong spread in the rest of the world. Phylogenetic studies subsequently revealed that the new virus, called H2N2, was the product of a reassortment of a H1N1 strain circulating in humans with an avian strain that contributed polymerase subunit 1 (PB1), hemagglutinin and neuraminidase coding genes. The peak of the epidemic in most European countries occurred in autumn 1957. Compared to the Spanish flu, mortality was significantly lower, with an estimated number of two million deaths and case-fatality rate below 0.2%. Excess mortality rates varied across countries, with the lowest observed in Europe and the highest in Latin America. Compared to previous years, mortality rate increased during pandemic in school-age children and young adults more than in the other age groups. In Italy, the cases peaked in October 1957 and it has been suggested that their actual number exceeded 8 million, i.e. one-sixth of the total Italian population at the time. However, from 1950 to 1957 no significant variation was observed either in the total number of deaths or in the annual death rates and the deaths occurred in 1957 were even fewer than in previous year. In Milan - the second largest city in Italy - over the three-year period from 1956 to 1958 an increase of just over 300 deaths was observed in 1957, compared with the approximately 140 expected. Deaths directly attributed to influenza were 178 out of the 28,020 deaths observed in the three-year period (6.3‰). Although Asian flu affected mostly young people and children worldwide, the majority of deaths attributed to influenza in Milan occurred among individuals over 55 years of age, predominantly males. Despite the large number of infections and deaths it caused, the impact of the new pandemic on mortality and global population growth has been limited and not comparable to with that of the 1918 pandemic. Nevertheless, Asian flu exerted a strong influence on healthcare organization worldwide. The new pandemic gave a strong final push towards overcoming the fragmentation of competences on health among different ministries with the establishment of the Ministry of Health in Italy.
Keywords: Influenza A virus, H2N2, Asian flu, Influenza pandemics, global health.
INTRODUCTION
The new flu emerged in the last months of 1956 in Guizhou, a southern province of China. By early February 1957, it had already spread to the rest of the country [1]. The rest of the world could learn about the new epidemic at the end of February, when the disease appeared in Singapore. On April 17, the New York Times reported that in Hong Kong, the flu has already affected more than 250,000 people in a short time [2]. The viral strain responsible of the new “Asian flu” was rapidly identified and proved to be distinct from those circulating in previous years [3]. A few weeks after the outbreak in Hong Kong, the new virus was isolated in London, Melbourne, and Washington, D.C. and it was decided to name it A2, to distinguish it from earlier influenza A strains. Only in 1971, following the revision of the nomenclature based on the characteristics of viral hemagglutinin and neuraminidase, it was named H2N2 [4, 5]. Phylogenetic studies subsequently revealed that H2N2 was the product of a genetic reassortment between strains circulating in humans in previous years, which contributed five of the eight viral genes, and an avian virus that contributed three new genes, the polymerase subunit PB1 and those encoding hemagglutinin and neuraminidase. The reassortment likely occurred between two and six years prior to the onset of the pandemic [6].
By late spring 1957, the world was therefore facing a new influenza pandemic, the first in history in which physicians and scientists could quickly detect it was caused by a new viral subtype, distinct from those previously circulating.
TOWARDS EUROPE AND IN ITALY
With few exceptions, the pandemic spread following land and sea routes, as air travel was still playing a minor role at the time. Singapore was an important hub for the virus spread to the rest of the world, as reported in a figure published in 1958 by the United Nations Educational, Scientific and Cultural Organization (UNESCO) (Figure 1). By the end of May 1957, an article in The Times of London reported the presence of suspected cases on a ship coming from the East docked in Rotterdam and expressed strong fears that the virus could invade Europe. However, this alarm was mitigated by reassuring about the prognosis: the flu in Asia would be mild in nature and would not cause death except in exceptional circumstances. This article was later cited by the Italian newspaper Corriere della Sera on May 31th, which acknowledged that it was impossible not to make a comparison with the terrible epidemic of 1918-19, that had started in a benign form. Again, according to The Times, it was emphasized that medical authorities had to remain vigilant because the danger could become serious and there were no suitable vaccines to fight the virus. [7]. In Italy, the Asian flu landed in Naples in August. In Bagnoli, over three hundred soldiers fell ill, and Naples itself was heavily affected, so much so that it was said that one in three Neapolitans was in bed with the flu. The virus quickly moved up the peninsula, dashing the hopes of those who were confident that its spread would be limited to the warmer months. On August 21st, the Corriere della Sera headlined “Cases of Asian flu also reported in Milan. The virus was imported from Naples”. The train from Naples – the so-called “direttissimo” – was blamed for the bringing the disease to the city. An article on August 31st in the same newspaper reported that in a barracks near Rome there were 700 cases of Asian flu and municipal authorities were somewhat apprehensive about the course of the epidemic in view of the reopening of schools. On September 21, the Corriere della Sera wrote that “Asian flu is spreading in Rome in an increasingly worrying manner” and that the 350 daily cases officially registered by the municipal health office had to be considered only a minimal part of the actual number. Since the beginning of August, 15,000 Romans had been “struck by the disease”. Meanwhile, absences from jobs in ministries, banks, and factories were significantly rising, some deaths were being observed, and in Tivoli, where a third of the population had been affected; “all the hospital beds are full”, so much so that the hospital management requested that school classrooms be used to accommodate the sick. In the Abruzzo National Park - therefore far from the most densely populated areas - the Asian flu affected a third of the inhabitants of Barrea and many residents of Pescasseroli. Reports of cases among military personnel were frequent, so much that it seems that the return to their homes of soldiers on leave may have played a significant role in spreading the epidemic along the peninsula. As example, thirteen recruits brought the disease in Cremona at the beginning of September. If barracks were therefore confirmed as a key site for airborne infection spread, seaside summer camps also played their part. In Marina di Massa, for example, 1500 children were affected in August [7].
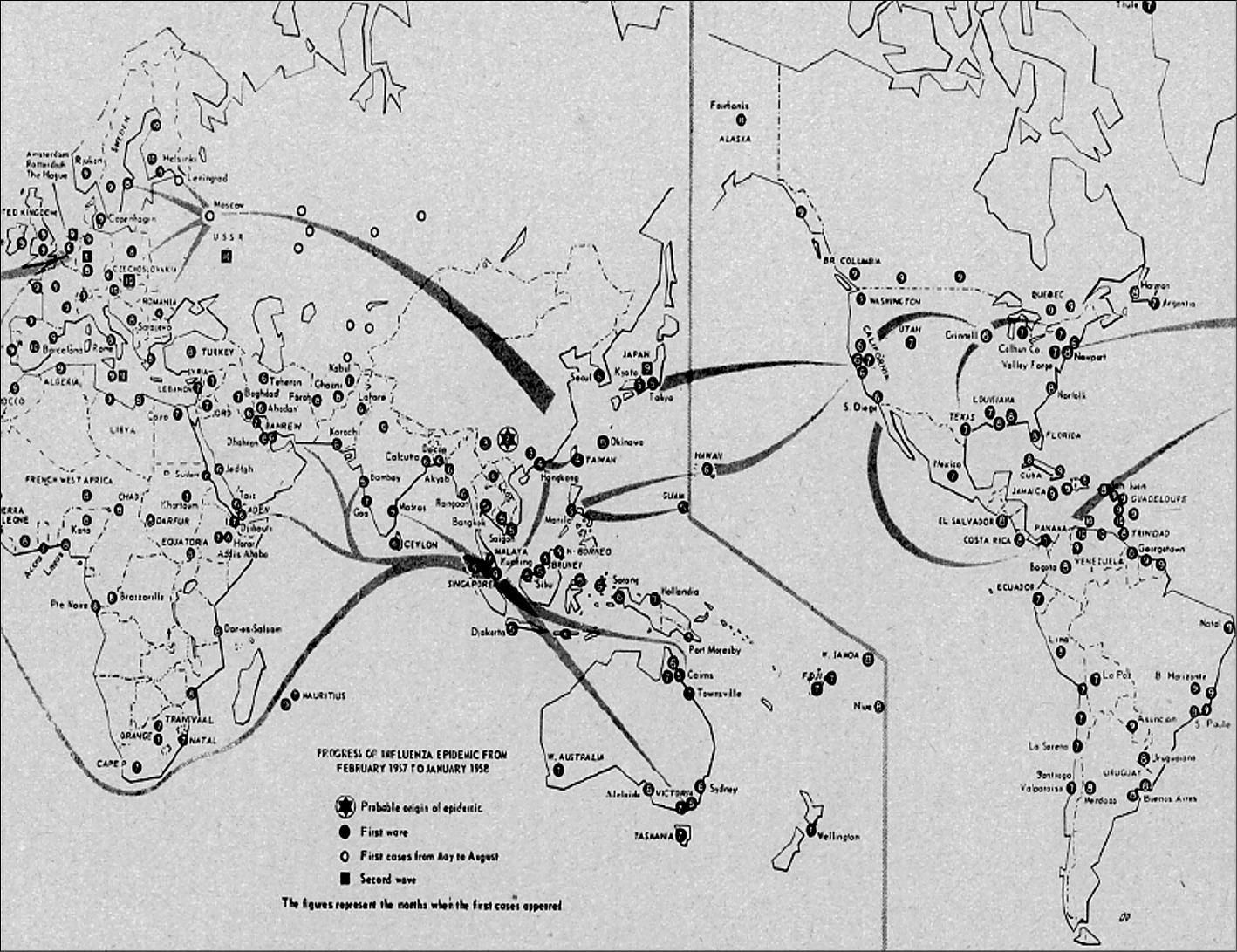
Figure 1 - The spread of Asian flu according to a map published by UNESCO in 1958.
During the fall of 1957, school reopening triggered wider transmission worldwide. Attack rates of 40-60% were observed among school children in the United States [8]. Data from Great Britain showed that the majority of those affected were in the 5-39 age group, with 49% of cases in 5-14 age group. In London, the number of absences from school grew rapidly, reaching 110,000. The nine years old Prince Charles was also in bed with the flu at the infirmary of the school he attended, where 80 out of 93 pupils had been affected. Adults who fell ill were mostly parents, teachers, and doctors. On September 30th, the Corriere della Sera reported that, due to the Asian flu outbreak, primary and lower secondary schools “would not reopen before the second half of October”. The article further noted that “although no directive had been issued by the central authorities”, most of the education authorities deemed it appropriate to implement emergency measures, fearing that the return of children to the classrooms might further exacerbate the epidemic. In Genoa, where the situation was particularly critical, the opening of primary and lower secondary schools was postponed until October 21st.
THE EPIDEMIC
The peak of the epidemic in most European countries occurred in autumn 1957. In Italy, the official data collected by the High Commissioner for Hygiene and Health are to be regarded as largely incomplete. According to available evidence, the peak was reached in October, and the disease slowly died out during the following spring [11, 12]. However, the 2,035,000 official reported cases (Figure 2) are certainly fewer than the actual ones. In the last four months of 1957, the National Institute for Health Insurance (INAM) certified 4,529,655 cases, and 6,180,345 over the entire eight-month period, therefore more than three times the number of official reports. Since this number is equal to 33% of the insured population – and considering that INAM assisted approximately three-quarters of Italy’s inhabitants – Giovanni Cavina, a contemporary author suggested that the actual number of cases exceeded 8 million, i.e. one-sixth of the total Italian population at the time, equivalent to 16,666 cases per 100,000 inhabitants. This estimate would be lower than what can be inferred from the available data for England [11].
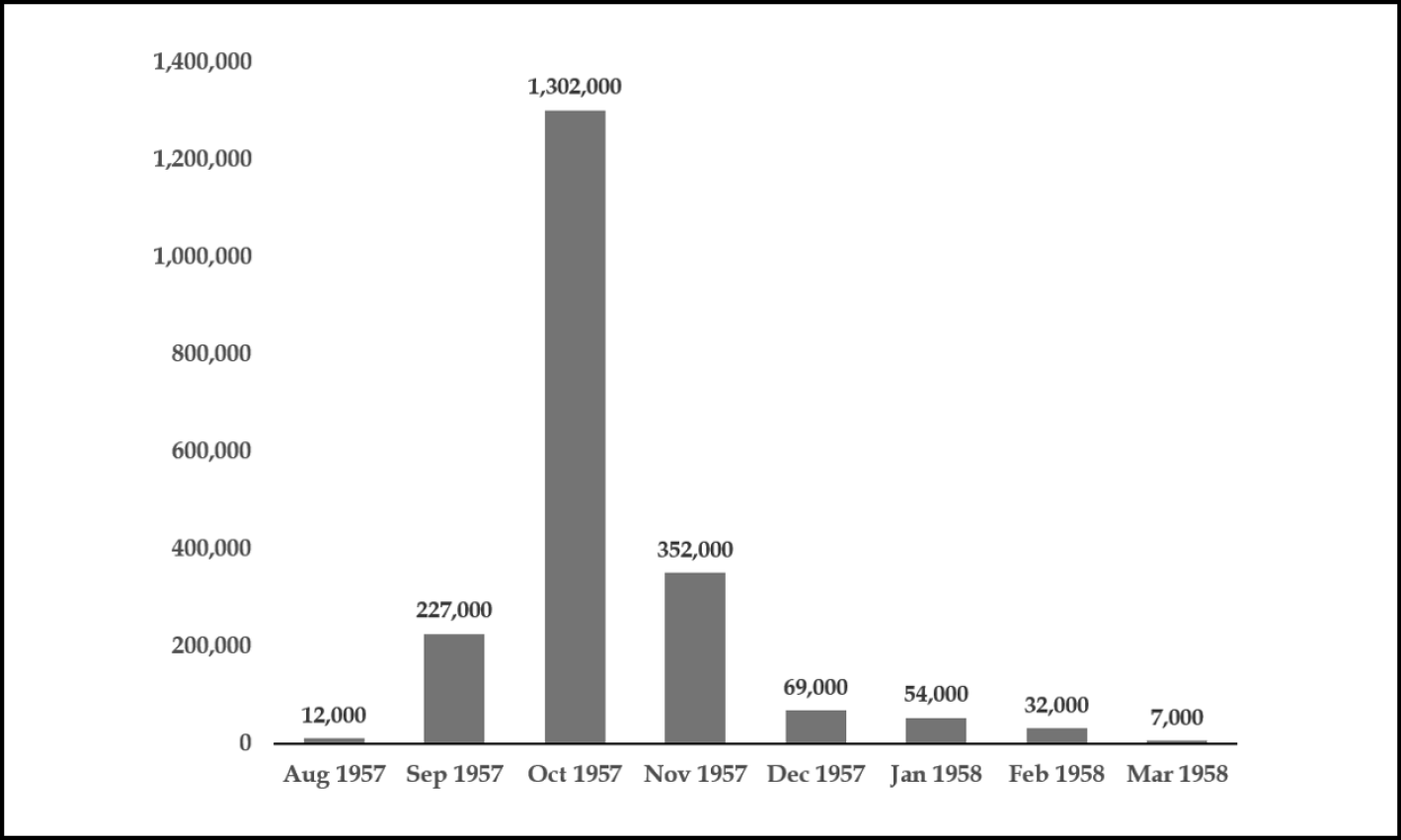
Figure 2 - Asian flu cases by month in Italy, 1957-1958: official reports.
On October 31st, 1957, the Corriere della Sera reported that, according to the prefecture of Rome, since September 26 and therefore in just over a month “5,490 cases of epidemic influenza had been confirmed in the capital, distributed as follows: in private homes 3,839, of which 156 required hospitalization...”. This 4% of hospitalization tells us about a disease that cannot be considered so mild. However, compared with the events of 1918, cases of viral interstitial pneumonia during the Asian flu were fewer and occurred mainly, although not exclusively, in patients with cardiopulmonary comorbidities. Among the cases studied at a hospital in New York, factors associated with an increased risk of developing primary viral pneumonia were having a history of rheumatic heart disease or being in the third trimester of pregnancy [13]. With regard to other risk factors, in Italy a high case-fatality rate was observed when influenza co-occurred with measles in children or with tuberculosis across all age groups [14].
During the most acute phase of the pandemic, sick leave was expected to weigh on production activities. The Corriere della Sera (28 November 1957) reported the Italian Chamber of Commerce data for the month of October, showing that the Asian flu had repercussions on industrial activities, particularly in the manufacturing sectors. Nevertheless, production remained high in the majority of basic industries, including heavy sectors such as steel, metallurgy and various branches of mechanics. In agriculture, a relatively favourable outcome for the autumn harvests was expected. Although somewhat ambiguous, this report was not in contrast with those based on more consistent data from the United States, where work absenteeism ranged between 3 and 8% at the peak of the pandemic, and the reduction in industrial production was limited to about 1%, followed by an almost immediate recovery [7]. Nonetheless, the costs of the pandemic were very high. According to Cosmacini, a rough estimate places the health burden at approximately 32 billion of lire [12].
Compared to the Spanish flu, mortality attributable to the Asian flu was significantly lower, with an estimated total number of two million deaths. The WHO estimated between one and four million deaths with a case-fatality rate below 0.2% [15]. Some studies attributed to the disease a mortality rate of around 0.3% in the United Kingdom [16], and data from 39 countries allowed to estimate an overall excess of deaths between 1957 and 1959 of 1.1 million, with a 95% confidence interval of 0.7 million to 1.5 million [17]. In this study, the average excess mortality rate for respiratory diseases associated with the pandemic was 1.9 per 10,000 inhabitants (95% CI 1.2 to 2.6). Across countries, excess mortality rates could vary as much as 70-fold, with the lowest rates observed in Europe and the highest in Latin America. Excess mortality was delayed by 1–2 years in 18 countries (46%). Compared with previous years, increases in mortality rate were proportionally greater in school-age children and young adults. Table 1 reports all causes mortality data in Italy from 1950 to 1960 (source the National Institute of Statistic, ISTAT), and shows no significant variation either in the total number of deaths or in the annual death rates in the entire period. In a rapidly growing population - over 2 million more inhabitants from 1950 to 1957 - the deaths in 1957 were even fewer than in previous year.
Table 1 - Total number of deaths and mortality rate per year in Italy from 1950 to 1959 (data from ISTAT).
|
Year |
Total population |
Total deaths |
Death rate ‰ |
|
1950 |
46,914,000 |
455,619 |
9.7 |
|
1951 |
47,295,000 |
485,208 |
10.3 |
|
1952 |
47,540,154 |
477,894 |
10.1 |
|
1953 |
47,792,434 |
476,015 |
10.0 |
|
1954 |
48,121,059 |
441,897 |
9.2 |
|
1955 |
48,476,568 |
446,689 |
9.2 |
|
1956 |
48,788,971 |
497,550 |
10.2 |
|
1957 |
49,051,924 |
484,190 |
9.9 |
|
1958 |
49,310,541 |
457,690 |
9.3 |
|
1959 |
49,639,684 |
454,740 |
9.2 |
MORTALITY IN MILAN IN THE YEARS OF ASIAN FLU PANDEMIC
In Italy, the civil registry office (the ‘Anagrafe’) was established in 1864 and subsequently regulated by a law enacted in 1954. The data reported below have been extracted from the Statistic Yearbook of the municipality of Milan, which offer the opportunity to compare what happened in the country’s second largest city with national data during the Asian flu pandemic. The total population of Milan in 1956 is estimated at 1.4 million inhabitants, and was growing rapidly, with a further increase of approximately 100,000 residents over the three-year period from 1956 to 1958. There is therefore no evidence of a negative impact of Asian flu on population growth. Figure 3 shows the total number of deaths observed over the three-year period and highlights an increase of just over 300 deaths in 1957, compared with the approximately 140 expected considering the increase in population. More of 80% of these excess deaths occurred among males. Deaths directly attributed to influenza amounted to a total of 178 out of the 28,020 deaths observed in the three-year period (6.3‰) (Figure 4). In all cases, it can be assumed that the diagnosis was based on clinical assessment and that the impossibility of obtaining laboratory confirmation induced many doctors to certify pneumonia or acute bronchitis as the cause of death rather than Asian flu. However, the number of deaths attributed to influenza increased sharply in 1957 compared with the previous year and rose by a few more units in 1958, suggesting that the attention aroused by the pandemic may have encouraged physicians to attribute a greater number of deaths to influenza. Despite the fact that the numbers are too small and probably not sufficiently representative of the actual mortality attributable to influenza to draw any conclusion, a slight prevalence of cases can be observed in the male sex in 1957 and in the female sex in 1958. Although Asian flu affected mostly young people and children worldwide [18], it should be noted that the majority of deaths attributed to influenza in Milan occurred among individuals over 55 years of age, predominantly males. Overall, deaths attributed to respiratory diseases showed an increase of 111 cases in 1957 in comparison with the previous year (Figure 5). Accordingly, a study aimed at assessing excess mortality rates in Australia, Canada, France, Japan, the UK, and the USA, reported an increase in mortality among the oldest age groups several seasons after both the A(H2N2) and A(H3N2) pandemics [19]. To further examine the reported potential impact of influenza on the course of tuberculosis, the number of deaths from TB in the years under study was also considered (Figure 6). A slight increase in TB deaths was recorded in 1957, with a return to 1956 levels in the subsequent year. Almost all of the increase was observed in males.
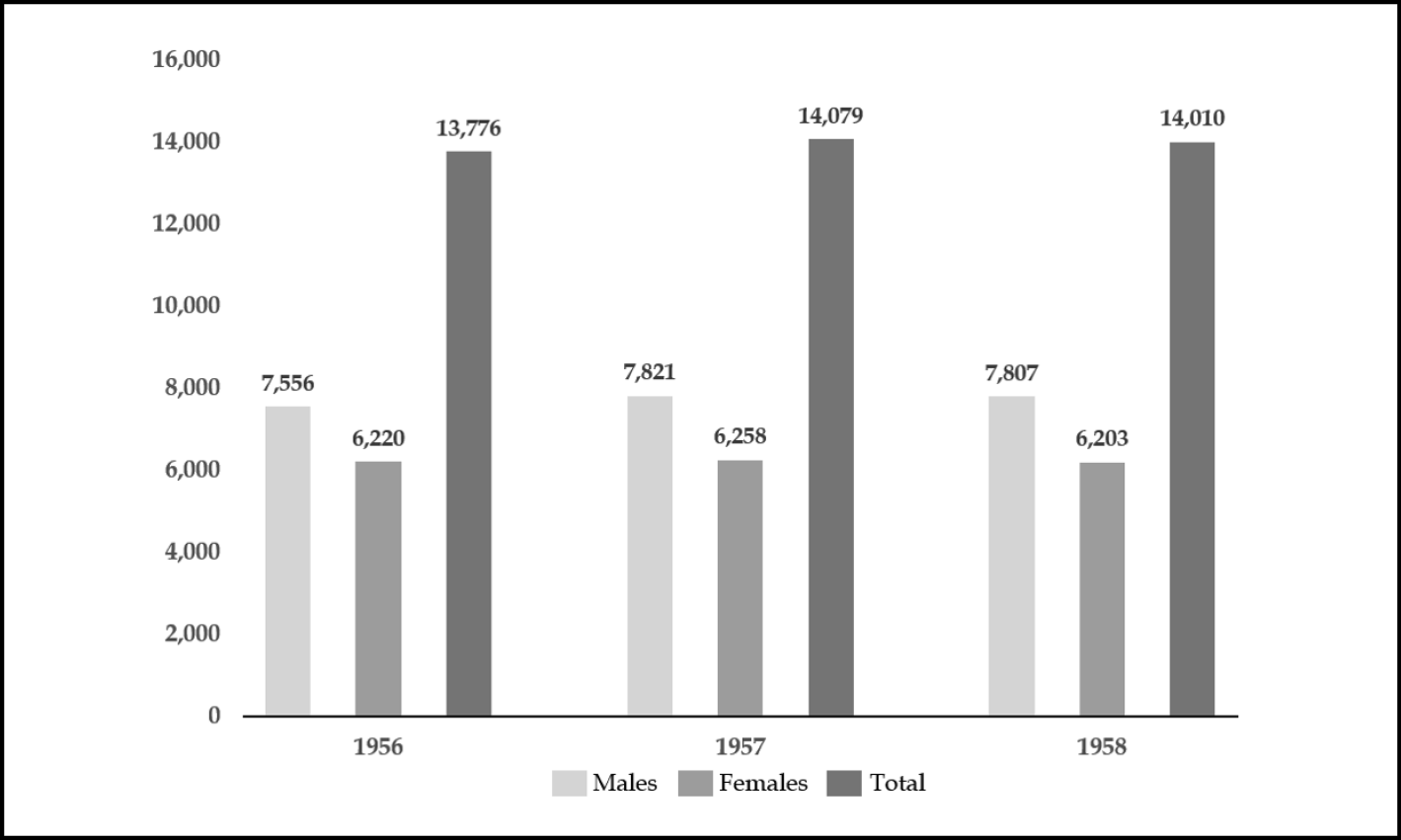
Figure 3 - Deaths from all causes recorded in Milan in the three-year period 1956-58 in males and females.
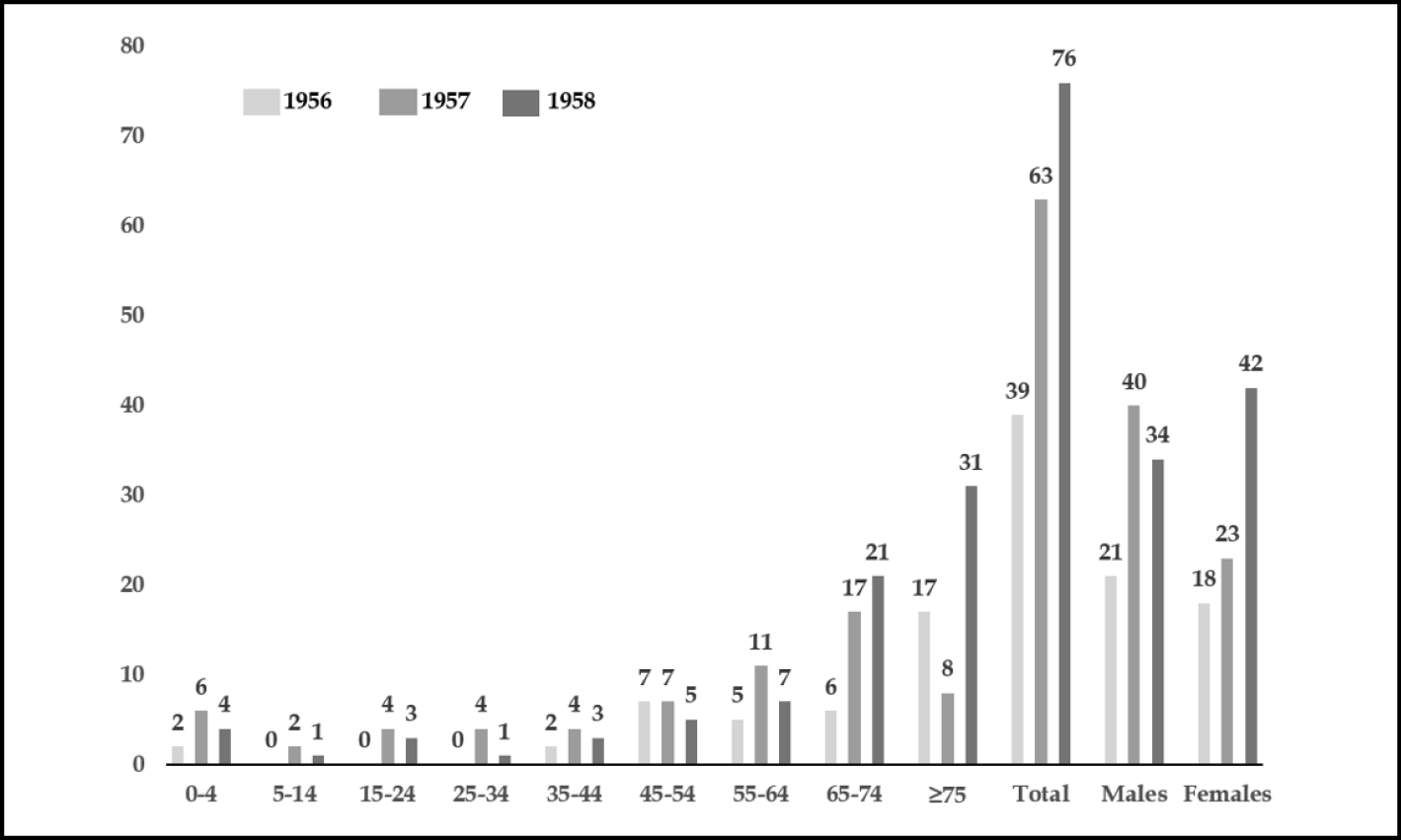
Figure 4 - Number of deaths by age group attributed to influenza in Milan in the three-year period 1956–1958.
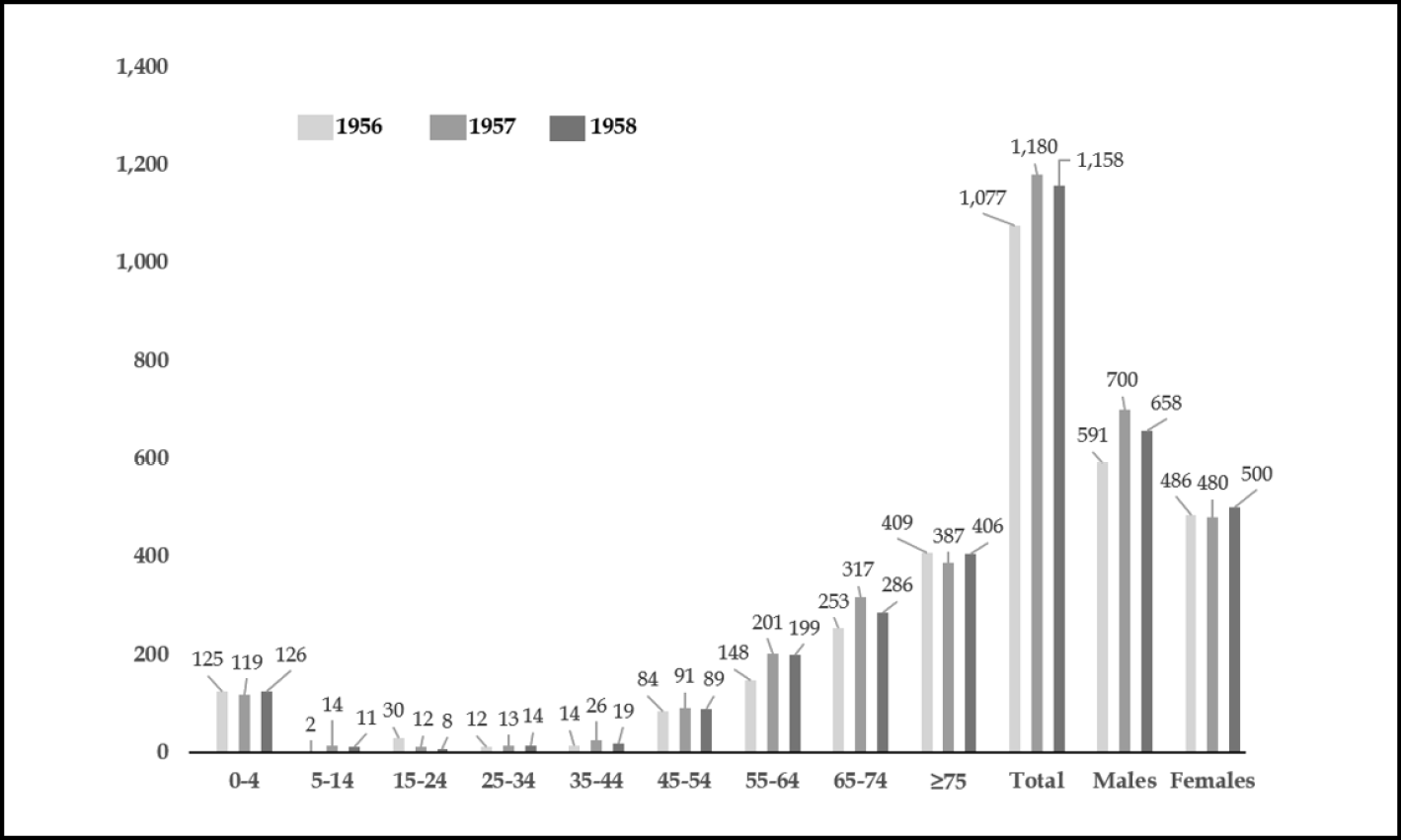
Figure 5 - Number of deaths by age group attributed to respiratory diseases in Milan during the three-year period 1956–1958. Deaths attributed to influenza are included.
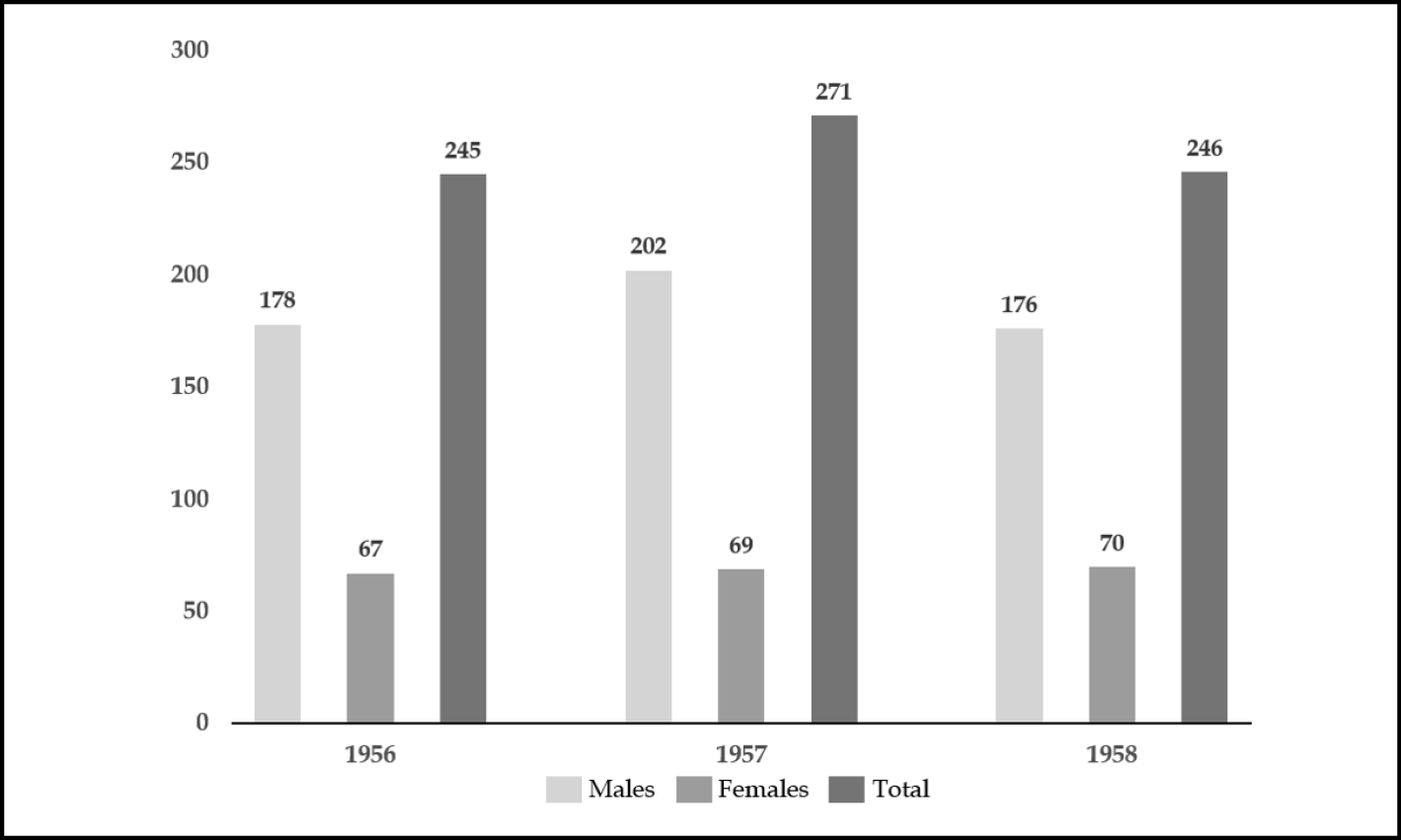
Figure 6 - Deaths from tuberculosis in Milan, years 1956-58.
LESSONS LEARNED AND CONCLUSIONS
The Asian flu provided the first demonstration of the influenza A virus’s attitude to change and the substantial unpredictability of the emergence of a new pandemic strain. The unpredictable transmission of avian viral strains to humans, as well as their potential reassortment with strains already circulating in human population is illustrated by numerous contemporary examples. The most striking concerns H5N1, which, over the course of nearly thirty years, has failed to adapt to sustained human-to-human transmission despite having infected humans on many occasions [20]. The 1951 virus, despite its wide spread and lethality, resembling those of a new pandemic virus [21], was still a H1N1 strain, descended from the 1918 Spanish flu virus. This observation has called into question the possibility of classifying influenza epidemics of the past as new pandemics based on mortality and geographical spread. The H2N2 subtype continued to circulate until 1968, when a new pandemic virus replaced it. Since its appearance, the H2N2 subtype generated new variants responsible for important epidemics in the early months of 1963 and during the winter of 1967-68, just a year before the emergence of the new pandemic virus H3N2 [21, 22].
In many parts of the world, the Asian pandemic exerted a stronger influence on healthcare systems than did the 1918 pandemic. In fact, although the Spanish flu had raised serious concerns about the adequacy of health systems, the demands imposed by the first world war had put health problems on the back burner [23, 24]. After the war, the pandemic became the subject of a “conspiracy of silence”, an attempt to erase it from collective memory in which the governments of industrialized countries, having proved unable to contain it, were heavily implicated [7, 23-26]. During the Asian pandemic, a still rudimentary surveillance and tracking system was tested for the first time in the United States [27]. In Italy, the pandemic led to discharge the proposal of the exclusion from welfare contributions of the so-called “small risk” - including short-term illnesses such as flu - which had been outlined to prevent welfare institutions from bankruptcy. The demonstration of how much a flu could determine a great risk, especially but not only, in the elderly and fragile subjects, had shown how wrong could be such a decision. Moreover, the limitations to the effectiveness of interventions due to the fragmentation of competences on health among different ministries, which had already proved detrimental during the Spanish flu, gave a strong final push towards the establishment of the Ministry of Health under the law of March 13, 1958 [7].
Despite the large number of infections and deaths it caused, the impact of the new pandemic on mortality and global population growth was limited and not comparable to that of the 1918 pandemic. Nevertheless, the press and governments emphasized its relative ‘mildness’, contributing to an underestimation of the pandemics as public health threat, an attitude that persisted for decades until crossing the threshold of the current century.
Funding
None
Conflict of interest
None
Acknowledgments
We would like to thank the Councillor Gaia Romani of the Milan City Council and Francesco Pizzorni of the Department of Civic Services of the Municipality of Milan.
REFERENCES
[1] Symposium on the Asian Influenza Epidemic, 1957. Proc Royal Soc Med. 1958; 51:1009-1018.
[2] Hong Kong battling influenza epidemic. The New York Times. April 17, 1957, p. 3.
[3] Langmuir A.D. Epidemiology of Asian influenza, international conference on Asian influenza. American Rev Resp Dis. 1961; 83: 2-14.
[4] A revised system of nomenclature for influenza viruses. Bull World Health Org. 1971; 45: 119-124.
[5] A revision of the system of nomenclature for influenza viruses: A WHO memorandum. Bull World Health Org 1980; 58: 585-591.
[6] Smith GJ, Bahl J, Vijaykrishna D et al. Dating the emergence of pandemic influenza viruses. Proc Natl Acad Sci U S A. 2009; 106(28): 11709-11712.
[7] Galli M. Una banale influenza? Storia di una malattia sottovalutata. Raffaello Cortina Editore. 2023; p 179-193.
[8] Carey DE, Dunn FL, Robinson RQ et al. Community-wide epidemic of Asian strain influenza: Clinical and subclinical illnesses among school children. JAMA. 1958; 167(12): 1459-1463.
[9] Ministry of Health. The influenza epidemic in England and Wales. 1957–1958. Rep Public Health Med Sub. 1960; 100: 13.
[10] Jackson C. History lessons: The Asian flu pandemic. Br J Gener Pract. 2009; 59(565): 622-623.
[11] Cavina G. L’influenza epidemica attraverso i secoli, Edizioni Pozzi, Roma. 1959; 221-222.
[12] Cosmacini G. Storia della medicina e della sanità nell’Italia contemporanea, Laterza, Roma-Bari. 1994; 40.
[13] Louria DD, Blumenfeld HL, Ellis JT, Kilbourne ED, Rogers DE. Studies on influenza in the pandemic of 1957-58. II. Pulmonary complications of influenza. J Clin Invest. 1959; 38: 213-265.
[14] Valenti S, De Palma M, Sternini M, et al. Nuovi casi di tubercolosi polmonare durante la recente epidemia influenzale A/S/1/57. Riv Tuberc App Resp. 1958; 6: 472.
[15] Pandemic Influenza Risk Management. who Interim Guidance, Genève 2013
[16] Henderson DA, Courtney B, Inglesby TV, Toner E, Nuzzo JB. Public health and medical responses to the 1957-58 influenza pandemic. Biosecur Bioterror. 2009; 7(3): 265-73.
[17] Viboud C, Simonsen L, Fuentes R, Flores J, Miller MA, Chowell G. Global mortality impact of the 1957-1959 influenza pandemic. J Infect Dis. 2016; 213: 738-745.
[18] Cox NJ, Subbarao K. Global epidemiology of influenza: Past and present. Ann Rev Med. 2000; 51: 407–421.
[19] Reichert T, Chowell G, McCullers JA. The age distribution of mortality due to influenza: pandemic and peri-pandemic. BMC Med. 2012; 10: 162.
[20] Galli M, Giacomelli A, Lai A, Zehender G. H5N1 influenza A virus: lessons from past outbreaks and emerging threats. Infez Med. 2025; 33(19): 76-89.
[21] Brüssow H. The beginning and ending of a respiratory viral pandemic-lessons from the Spanish flu. Microb Biotechnol. 2022; 15: 1301-1317.
[22] Noble GR, “Epidemiological and clinical aspects of influenza”, in A.S. Beare, Basic and Applied Influenza Research, CRC Press, Boca Raton, FL. 1982; 11-50.
[23] Goldstein JL. The Spanish 1918 Flu and the COVID-19 Disease: The Art of Remembering and Foreshadowing Pandemics. Cell. 2020; 183(2): 285-289.
[24] Radparvar S. From Black Death to COVID-19: Lessons Learned from the Past Pandemics. Infez Med. 2025; 33 (4); 461-474.
[25] Tognotti E. La Spagnola in Italia. Franco Angeli, Milano, II ed. 2015, p. 85.
[26] Spinney L. Pale Rider. Jonathan Cape, 2017.
[27] Henderson D. The development of surveillance systems. Am J Epidemiol. 2016; 183; 381-386.