Le Infezioni in Medicina, n. 2, 227-232, 2026
doi: 10.53854/liim-3402-12
CASE REPORTS
Refractory XDR Klebsiella pneumoniae CAUTI Treated with non-antibiotic urinary acidification: a 12-month follow-up case report and literature review
Merin Anna Job¹, Manu Dius Kandachamkulam², Dani Dius Fernandes³
1Department of General Medicine, Government Medical College, Thiruvananthapuram, Kerala, India;
2Department of General Medicine, AJ Hospital, Thiruvananthapuram, Kerala, India;
3Department of Internal Medicine, King Saud Medical City, Riyadh, Saudi Arabia.
Article received 6 February 2026 and accepted 8 April 2026
Corresponding author
Merin Anna Job
E-mail: merin.shiju@gmail.com
SUMMARY
Background: The increase of catheter-associated urinary tract infections (CAUTIs) caused by extensively drug-resistant (XDR) Klebsiella pneumoniae represents a critical failure of the current antimicrobial paradigm. In geriatric cohorts with significant comorbidities, the exhaustion of conventional therapeutic options often precipitates a cycle of recurrent sepsis, prolonged hospitalization, and prohibitively high healthcare expenditure. When “last-resort” agents such as ceftazidime-avibactam and colistin fail, clinicians in resource-limited settings are left with no guideline-endorsed alternatives. This report evaluates the clinical and economic impact of a pragmatic non-antibiotic acidification strategy applied as a salvage intervention in a “pan-resistant” scenario.
Case Report: We describe the complex clinical course of an 82-year-old female with type 2 diabetes and neurogenic bladder following an acute ischemic stroke. Despite rigorous adherence to standard catheter care protocols, she developed intractable, recurrent XDR K. pneumoniae CAUTI. The pathogen demonstrated resistance to all first-line and reserve antibiotics, leading to four ICU admissions within a single trimester. With methenamine hippurate unavailable and the family declining suprapubic diversion, we initiated a physiological acidification protocol. This regimen synergized high-dose oral ascorbic acid (2g/day) - hypothesized to downregulate virulence genes - with twice-daily bladder irrigation using diluted (0.25%) acetic acid to create a hostile pH environment for bacterial adherence.
Literature Search Methods and Results: Utilizing PRISMA principles adapted for narrative synthesis, a systematic search of PubMed and Scopus yielded 145 initial results. After screening for relevance to non-antibiotic salvage therapy and biofilm disruption, 17 highly relevant articles were incorporated to validate the mechanistic plausibility of our combined protocol.
Conclusions: Following initiation of the intervention, a sustained absence of symptomatic episodes was observed. Over a 12-month follow-up, the patient remained free of CAUTI, requiring no further antibiotic therapy. We posit that low-cost, accessible acidification adjuncts represent a vital “frugal innovation” for antimicrobial stewardship in vulnerable populations.
Keywords: Klebsiella pneumoniae, urinary acidification, biofilm, CAUTI, case-report.
INTRODUCTION
Catheter-associated urinary tract infections (CAUTIs) are among the most prevalent healthcare-associated infections globally, imposing a substantial burden on patient safety and healthcare economics. The management of these infections is increasingly complicated by the rapid proliferation of multidrug-resistant (MDR) and extensively drug-resistant (XDR) Gram-negative pathogens. Globally, Klebsiella pneumoniae infections cause approximately 800,000 deaths annually, with resistance to cephalosporins and carbapenems driving over 50% of this mortality [1]. In South Asia and other resource-constrained settings, the epidemiology is shifting alarmingly. Longitudinal surveillance data indicates a sustained rise in resistance to cornerstone agents among community and hospital isolates [2]. This crisis is exacerbated by the increasing burden of metallo-beta-lactamase-producing Enterobacterales, which profoundly restrict therapeutic avenues and worsen clinical outcomes [3].
K. pneumoniae is particularly notorious in this context due to its ability to form dense biofilms on catheter surfaces. Biofilms encase bacteria in a protective extracellular matrix, significantly reducing the penetration of antimicrobial agents and rendering standard susceptibility testing unreliable [4]. Consequently, clinicians frequently encounter scenarios where in-vitro susceptibility does not translate to in-vivo cure, leading to a cycle of relapse and escalation to toxic “last-resort” antibiotics [5]. This reflects a broader global erosion of oral antibiotic efficacy, particularly among fluoroquinolones, which has severely compromised outpatient management strategies for urinary isolates [6, 7]. The loss of these oral options often forces unnecessary hospitalization for intravenous therapy, increasing both cost and resistance risks [8]. The economic and psychosocial impact of this cycle is profound, driving up healthcare costs through prolonged admissions and loss of caregiver productivity, a burden disproportionately felt in developing economies [9].
Furthermore, repeated courses of broad-spectrum antibiotics devastate protective endogenous microbiomes. As recently highlighted by Moriconi et al., maintaining physiological environments that support native flora is crucial in counteracting urinary tract infection occurrences and recurrences [10]. When conventional antibiotic strategies fail, and when alternative antiseptics like methenamine hippurate are locally unavailable, there is a critical need for “frugal innovations”—low-cost, physiologically plausible interventions that can disrupt biofilms without exerting antimicrobial selective pressure. We present a case of refractory XDR K. pneumoniae CAUTI in a geriatric patient, successfully managed with a non-antibiotic protocol combining bladder irrigation (acetic acid) and urinary acidification (Vitamin C).
CASE REPORT
An 82-year-old female with type 2 diabetes presented with progressive obtundation and hemodynamic instability, necessitating Intensive Care Unit (ICU) admission. She was diagnosed with an acute ischemic stroke complicated by aspiration pneumonitis and septic shock. Due to urinary retention and the need for strict output monitoring, an indwelling latex Foley catheter was inserted. The patient was managed with intravenous ceftriaxone, antiplatelet therapy, and supportive care.
While her neurological and respiratory status stabilized, allowing ward transfer by day 5, she developed high-grade fever with rigors and turbid urine during convalescence. Urine cultures revealed MDR K. pneumoniae resistant to all first-line antibiotics including piperacillin-tazobactam and meropenem. The indwelling latex catheter was immediately replaced with a 100% silicone catheter, and therapy was empirically escalated to ceftazidime-avibactam. Interestingly, a subsequent CARBA-R molecular assay demonstrated the presence of carbapenemase genes conferring genotypic resistance to ceftazidime-avibactam. However, the patient exhibited clinical defervescence, and the course was completed based on clinical response - a discordance likely attributable to the limitations of in-vitro testing in biofilm-mediated infections.
Following discharge, the patient entered a cycle of debilitating recurrences. Over the next three months, she suffered three further episodes of severe CAUTI. Episode 2 involved recurrence with Pseudomonas aeruginosa; episode 3 involved recurrence with XDR K. pneumoniae unresponsive to ceftazidime-avibactam and resistant to tigecycline, necessitating fosfomycin salvage therapy; episode 4 presented as severe pyelonephritis with macroscopic hematuria caused by a “pan-resistant” K. pneumoniae strain. This final episode required readmission and combination therapy with meropenem and colistin. By the end of the third month, the patient had undergone four hospital admissions. The cumulative antibiotic exposure was immense, and the organism had evolved into an XDR phenotype with no remaining oral therapeutic options. Suprapubic catheterization was offered but declined by the family. Crucially, methenamine hippurate, a standard urinary antiseptic, was not available in India.
Faced with a therapeutic dead-end, a multidisciplinary decision was made to trial a non-antibiotic, acidification-based prophylaxis protocol. The rationale was to create a hostile urinary environment for K. pneumoniae growth and biofilm maintenance. Written informed consent was obtained for this off-label approach. The regimen comprised systemic acidification using high-dose oral Ascorbic Acid (Vitamin C), 2g/day in divided doses, and local, twice-daily bladder irrigation with sterile diluted (0.25%) acetic acid. The solution was instilled via the catheter, retained for 30 minutes, and then drained. This was paired with a strict schedule of silicone catheter replacement every 21 days and dietary modification restricting alkalinizing foods. Urinary pH was monitored utilizing Combur-Test urine dipsticks (Roche Diagnostics). As no universally established target range exists in current literature, we conservatively targeted a pH of 6. Systematic monitoring of urinary pH was performed daily for the first 5 days until this target was achieved. Subsequently, monitoring was spaced to fortnightly for one month, and then maintained on a monthly basis. To monitor for potential systemic acidosis resulting from topical absorption, Arterial Blood Gases (ABGs) were monitored during the hospitalized duration. Following discharge, surveillance was transitioned to monthly Venous Blood Gases (VBGs) to specifically monitor pH and serum bicarbonate (HCO3) levels, alongside routine electrolytes.
Prior to the intervention, the patient’s primary caregiver reported severe psychosocial and financial distress. The unpredictability of the infections meant the caregiver was unable to maintain employment, and the financial strain of repeated ICU admissions was becoming untenable. The patient, formerly independent, developed significant anxiety related to catheter care, viewing the device as a source of constant “poison”. Following the initiation of the protocol, the primary caregiver was strictly trained in the aseptic irrigation technique and demonstrated competency before discharge. The active involvement empowered the family, and they noted the immediate disappearance of the foul urinary odor. “It gave us our life back,” the caregiver noted during the six-month follow-up.
The intervention was well-tolerated. The patient reported no suprapubic discomfort, burning sensation, or hematuria. Crucially, no metabolic acidosis was observed at any point during ABG or VBG monitoring. The follow-up regimen included monthly urine routine, urine cultures, renal function tests (RFTs), and serum electrolytes. Additionally, weekly telephone consultations were conducted to actively monitor for emerging clinical symptoms. Over the subsequent 12-month follow-up, the patient remained entirely free of symptomatic CAUTI. Routine surveillance cultures occasionally showed asymptomatic bacteriuria, but in the absence of fever or systemic symptoms, antibiotics were withheld. The hospitalization rate dropped to zero. The chronological sequence of clinical events, microbiological findings, and therapeutic interventions is summarized in Figure 1.
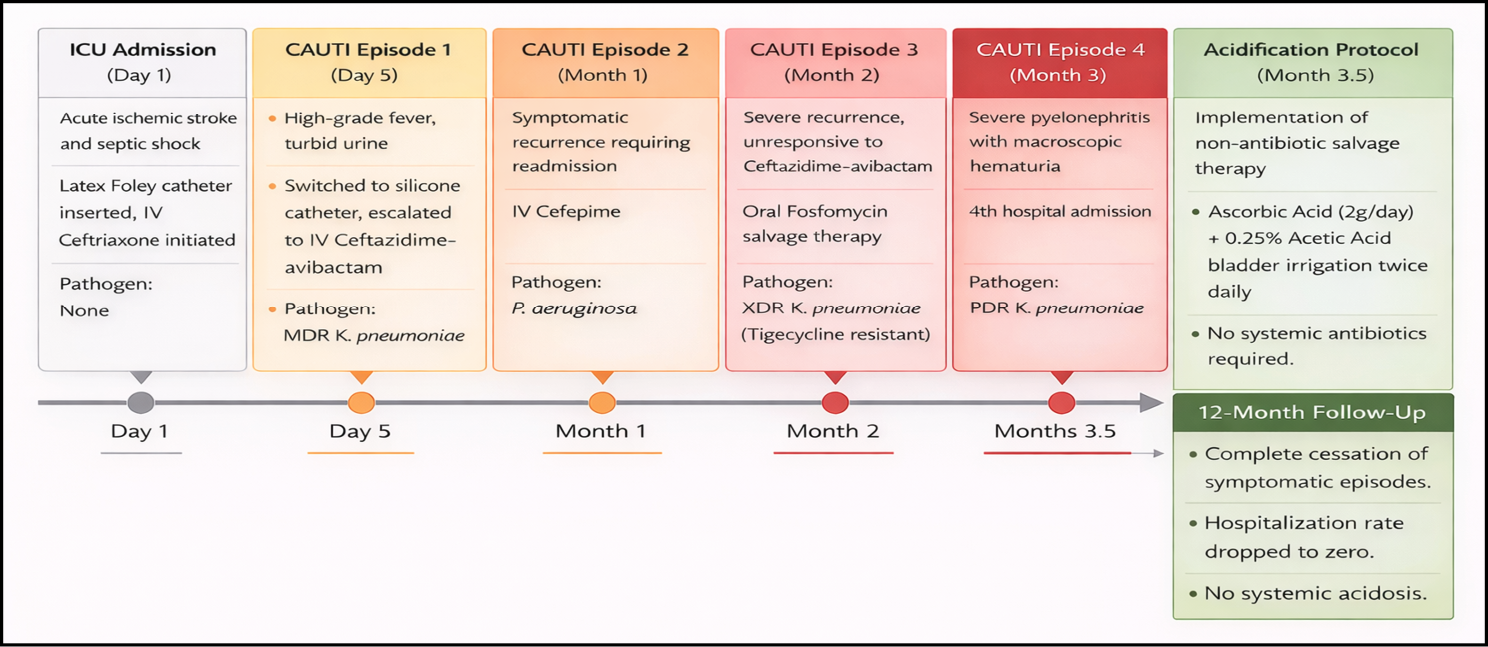
Figure 1 - Timeline of clinical course, microbiological findings, and therapeutic interventions in recurrent catheter-associated urinary tract infection.
Legend: Timeline depicting the progression of recurrent catheter-associated urinary tract infections, including clinical events, identified pathogens, and antimicrobial or non-antibiotic interventions over a 15-month period. The initiation of urinary acidification therapy is followed by sustained clinical remission without further hospitalizations.
Abbreviations: CAUTI, catheter-associated urinary tract infection; MDR, multidrug-resistant; XDR, extensively drug-resistant.
LITERATURE SEARCH METHODS
Guided by PRISMA principles for narrative synthesis, we searched PubMed/MEDLINE and Scopus for English-language literature (up to December 2025) using combinations of: “urinary acidification,” “ascorbic acid,” “acetic acid irrigation,” “biofilm disruption,” and “CAUTI.” From 145 initial results, articles were systematically screened for relevance to non-antibiotic salvage therapies, biofilm disruption, and multidrug-resistant CAUTI.
RESULTS OF THE LITERATURE SEARCH
Following full-text assessment, 17 relevant articles were included: 6 in-vitro mechanistic studies, 4 clinical observational studies, 3 randomized/quasi-experimental trials, and 4 case reports/series (Table 1). The extracted literature validates our combined acidification protocol along two principal mechanistic axes: (1) physicochemical disruption of biofilm integrity via local pH modulation, and (2) attenuation of bacterial virulence through altered gene expression and metabolic pathways. Importantly, these findings highlight a critical clinical gap. Despite strong biological plausibility and supportive early-phase data for acetic and ascorbic acid therapies, there remains a conspicuous absence of large-scale, controlled trials evaluating urinary acidification for XDR CAUTI. This lack of guideline-endorsed alternatives for pan-resistant scenarios reinforces the critical need for hypothesis-generating reports such as the present study.
Table 1 - Summary of Key Included Studies on Urinary Acidification.
|
Study Type |
No. of Studies |
Key Findings |
Representative References |
Relevance |
|
In-vitro mechanistic |
6 |
Anti-biofilm and anti-virulence effects |
[11] |
Biological plausibility |
|
Randomized/interventional |
3 |
Reduced bacteriuria with bladder irrigation |
[12, 13] |
Supports irrigation |
|
Observational |
4 |
Reduced recurrence with non-antibiotic adjuncts |
[14] |
Real-world relevance |
|
Case reports/series |
4 |
Success in salvage therapy |
[14, 15] |
Direct clinical parallel |
DISCUSSION
This case suggests the potential utility of a “back-to-basics” physiological strategy in the management of modern, highly resistant infectious diseases. The successful 12-month remission of an XDR K. pneumoniae infection using acetic acid and Vitamin C suggests a potential alternative to increasingly expensive and toxic reserve antibiotics. The efficacy of this regimen likely stems from a synergistic disruption of the bacterial biofilm, the primary defense mechanism of K. pneumoniae in CAUTI. Historic data supports the use of short-chain organic acids as antiseptics, as acetic acid penetrates bacterial cell walls, acidifying the cytoplasm and disrupting enzymatic functions [15]. A randomized controlled trial by Chung et al. showed that vinegar bladder irrigation significantly reduced bacteriuria in long-term catheterized patients, while Bruun et al. demonstrated the safety of this approach in reducing catheter encrustation [12, 13]. More recent reports reinforce its value as a salvage therapy when standard options fail or are unavailable [14].
While traditionally viewed merely as a urinary acidifier, recent transcriptomic evidence suggests Vitamin C exerts a more sophisticated mechanism. A pivotal study by Xu et al. demonstrated that Vitamin C exerts multifaceted anti-virulence activity against carbapenem-resistant K. pneumoniae. Mechanistically, it dissipates the bacterial proton motive force, thereby inhibiting the efflux pumps required to transport capsular polysaccharides to the cell surface [11]. Furthermore, the study confirmed that Vitamin C downregulates the expression of critical virulence genes, including the capsule regulators rmpA and rmpA2, biofilm-associated genes luxS and galF, and fimbrial adhesion genes fimB, mrkJ, and ecpA [11]. In our patient, we hypothesize that this synergistic blockade may have impaired the pathogen’s virulence mechanisms.
It is vital to acknowledge that acetic acid bladder irrigation is not currently endorsed by major urological guidelines (e.g., EAU, AUA) for routine prophylaxis. This caution is driven by theoretical risks of chemical cystitis, hematuria, and systemic acidosis resulting from mucosal absorption [16]. However, these guidelines largely assume the availability of effective alternatives. In the context of “pan-resistance,” where the alternative is septic shock or permanent nephrostomy, the risk-benefit calculus shifts. Our rigorous monitoring with daily pH tracking and ABG/VBG assessments confirmed the safety of this highly dilute (0.25%) solution, supporting previous findings in neurogenic bladder cohorts [14]. A notable feature of this case was the discordance between the CARBA-R assay and the initial clinical response. Standard susceptibility testing is performed on planktonic bacteria and fails to account for the biofilm mode of growth, which increases antibiotic tolerance by up to 1000-fold [4]. Conversely, this implies that agents which disrupt biofilms may restore clinical success even when the bacterium appears resistant by standard metrics.
The economic argument for this strategy remains compelling, particularly regarding the “financial toxicity” associated with antimicrobial resistance in the Global South. In India, where out-of-pocket expenditure accounts for over 50% of total health spending, the cost of reserve antibiotics can be catastrophic, frequently pushing families into poverty [9, 17]. By replacing these prohibitively expensive agents with a low-cost, home-based regimen, we achieved a massive reduction in direct healthcare costs.
As a single-case observation, this report cannot definitively establish causality. A key confounding variable was the transition from a latex to a 100% silicone catheter. While studies like Verma et al. show pure silicone significantly reduces early bacterial colonization compared to latex, our patient still suffered three severe recurrences post-switch, suggesting silicone alone was insufficient against these resistant isolates [18]. Furthermore, the acidification protocol was paired with a strict 21-day catheter replacement schedule, making it difficult to isolate whether prolonged remission was driven by physicochemical biofilm disruption or the accelerated exchange frequency. Finally, although rigorous monitoring revealed no adverse systemic effects, long-term mucosal tolerability requires validation in larger, prospective cohorts. Therefore, the 12-month clinical remission represents a strong temporal association rather than a proven direct therapeutic effect.
CONCLUSIONS
As the pipeline for new antibiotics slows and resistance mechanisms evolve, the medical community must look backward as well as forward. This approach merits serious consideration as a frugal innovation for refractory cases in resource-limited settings. We hypothesize that sustained urinary acidification disrupts biofilm stability while concurrently attenuating bacterial virulence pathways. Large-scale, multi-center, randomized controlled trials comparing acidification protocols against standard care in silicone-catheterized cohorts are warranted to formalize dosing protocols, confirm safety profiles, and justify guideline endorsement. This approach aligns with antimicrobial stewardship principles by reducing selective pressure and preserving the efficacy of last-resort antibiotics.
Funding
None.
Conflict of interest
The authors declare no conflict of interest.
Patient consent
Written informed consent was obtained from the patient’s legal representative for the publication of this case report. A copy of the consent form has been uploaded as supplementary file alongside this reviewed submission.
REFERENCES
[1] Song HW, Lin Y, Wan TE, et al. Global burden of Klebsiella pneumoniae infections and antimicrobial resistance in 2019. BMC Infect Dis. 2025; 25 (1): 1773.
[2] Kidwai SS, Nageen A, Ghaznavi S, et al. Antibiotic susceptibility in commonly isolated pathogens from urinary tract infection in a cohort of subjects from low socioeconomic strata. Pak J Med Sci. 2017; 33 (2): 254-259.
[3] Tiseo G, Stefani S, Fasano FR, et al. The burden of infections caused by Metallo-Beta-Lactamase-Producing Enterobacterales in Italy: epidemiology, outcomes, and management. Infez Med. 2025; 33 (3): 249-260.
[4] Sharma D, Misba L, Khan AU, et al. Antibiotics versus biofilm: an emerging battleground in microbial communities. Antimicrob Resist Infect Control. 2019; 8: 76.
[5] Zilberberg MD, Shorr AF. Secular trends in gram-negative resistance among urinary tract infection hospitalizations in the United States, 2000-2009. Infect Control Hosp Epidemiol. 2013; 34 (9): 940-946.
[6] Sanchez GV, Master RN, Karlowsky JA, et al. In vitro antimicrobial resistance of urinary Escherichia coli isolates among US outpatients from 2000 to 2010. Antimicrob Agents Chemother. 2012; 56 (4): 2181-2183.
[7] Zhanel GG, Hisanaga TL, Laing NM, et al. Antibiotic resistance in outpatient urinary isolates: final results from the North American Urinary Tract Infection Collaborative Alliance (NAUTICA). Int J Antimicrob Agents. 2005; 26 (5): 380-388.
[8] Dalhoff A. Global fluoroquinolone resistance epidemiology and implications for clinical use. Interdiscip Perspect Infect Dis. 2012; 2012: 976273.
[9] Zhu NJ, Weldegiorgis M, Carter E, et al. Economic burden of community-acquired antibiotic-resistant urinary tract infections: a systematic review and meta-analysis. JMIR Public Health Surveill. 2024; 10: e53828.
[10] Moriconi F, Pelagagge M, Bertini M. Vaginal microbiota and urinary tract infections in women: the protective role of vaginal lactobacilli in counteracting urinary tract infections occurrence and recurrence. Infez Med. 2026; 1: 39-48.
[11] Xu C, Dong N, Chen K, et al. Bactericidal, anti-biofilm, and anti-virulence activity of vitamin C against carbapenem-resistant hypervirulent Klebsiella pneumoniae. iScience. 2022; 25 (3): 103894.
[12] Chung YC, Chen HH, Yeh ML. Vinegar for decreasing catheter-associated bacteriuria in long-term catheterized patients: a randomized controlled trial. Biol Res Nurs. 2012; 14 (3): 294-301.
[13] Bruun JN, Digranes A. Bladder irrigation in patients with indwelling catheters. Scand J Infect Dis. 1978; 10 (1): 71-74.
[14] Moussa M, Chakra MA, Papatsoris AG, et al. Bladder irrigation with povidone-iodine to prevent recurrent urinary tract infections in neurogenic bladder patients on clean intermittent catheterization. Neurourol Urodyn. 2021; 40 (2): 672-679.
[15] Bachow BH. Intravesical acetic acid in combination with prophylactic methenamine and ascorbic acid to decrease the incidence of recurrent urinary tract infections associated with intermittent urinary self-catheterization: a case report. Urol Case Rep. 2020; 35: 101531.
[16] Pfizer Inc. Acetic Acid 0.25% Irrigation USP prescribing information. 2024. Available from: https://labeling.pfizer.com
[17] Farooqui HH, Karan A, Mathur MR, et al. Out-of-pocket expenditure on childhood infections and its financial burden on Indian households: Evidence from nationally representative household survey (2017-18). PLoS One. 2022; 17 (12): e0278025.
[18] Verma A, Bhani D, Tomar V, et al. Differences in bacterial colonization and biofilm formation property of uropathogens between the two most commonly used indwelling urinary catheters. J Clin Diagn Res. 2016; 10 (6): PC01-PC03.