Le Infezioni in Medicina, n. 2, 220-226, 2026
doi: 10.53854/liim-3402-11
ORIGINAL ARTICLES
Rezafungin and catheter-related candidemia: a new player in a high-stakes game
Sergio Venturini1, Ingrid Reffo2, Agnese Zanus-Fortes1, Giovanni Del Fabro1, Astrid Callegari1, Federico Giovagnorio1, Camilla Negri1, Mariateresa Casarotto3, Giancarlo Basaglia3, Chiara Zanusso4, Barbara Basso4
1 Department of Infectious Diseases, ASFO Santa Maria degli Angeli Hospital, Pordenone, Italy;
2 Department of Anesthesiology, ASFO Santa Maria dei Battuti Hospital, San Vito al Tagliamento, Pordenone, Italy;
3 Department of Microbiology, ASFO Santa Maria degli Angeli Hospital, Pordenone, Italy;
4 Pharmacy Service, ASFO Santa Maria degli Angeli Hospital, Pordenone, Italy.
Article received 5 March 2026 and accepted 23 April 2026
Corresponding author
Ingrid Reffo
E-mail: ingrid.reffo@asfo.sanita.fvg.it
SUMMARY
Candidemia remains a significant healthcare-associated infection characterized by high mortality rates and considerable resource utilization. While echinocandins are established as first-line treatment, extended daily intravenous administration often delays patient discharge, particularly when transitioning to oral azoles is not feasible. Rezafungin, a novel long-acting echinocandin, offers once-weekly dosing with predictable pharmacokinetics.
This prospective observational pilot study examined consecutive cases of guideline-defined catheter-related candidemia (CRC) diagnosed in medical wards at two Italian hospitals in 2025. All subjects initially received short-acting echinocandin therapy alongside catheter removal for source control. Upon meeting predefined clinical and microbiological stability criteria, patients were administered a single dose of rezafungin on day 7. Primary outcomes included clinical success and microbiological clearance at 30 days. Secondary endpoints encompassed reductions in hospital length of stay, relapse rates, mortality, and adverse drug events.
Seven patients received rezafungin as consolidation therapy. The cohort was characterized by advanced age and a high comorbidity burden. Microbiological eradication was achieved in all cases. No drug-related adverse events, relapses, or deaths were observed at 30- and 90-day follow-up. The median estimated decrease in hospital stay was four days, translating to 28 bed-days saved.
This real-world pilot cohort demonstrated that a stepwise antifungal strategy incorporating rezafungin following initial echinocandin therapy is feasible, well-tolerated, and associated with favorable short-term outcomes. Such an approach may facilitate earlier patient discharge, mitigate vascular-access issues, and support more efficient management of catheter-related candidemia. Larger, multicenter controlled studies are necessary to verify the clinical, economic, and sustainability benefits.
Keywords: rezafungin, catheter-related candidemia, single dose, long-acting antifungal.
INTRODUCTION
Candidemia remains a serious healthcare-associated infection causing high morbidity, mortality, and resource use, especially among elderly patients or in presence of risk factors [1-4]. Management is complex, requiring prolonged intravenous (IV) therapy and comprehensive diagnostic and therapeutic assessment [1, 5, 6].
Echinocandins are recommended as first-line therapy owing to their efficacy, favorable safety profile, and limited drug-drug interactions [5]. According to the 2025 global guidelines of the European Confederation of Medical Mycology (ECMM), the International Society for Human and Animal Mycology (ISHAM), and the American Society for Microbiology (ASM), candidemia without deep-seated organ involvement requires 14 days of treatment after the first persistently negative blood culture. Oral azole step-down may be considered in clinically stable patients with documented bloodstream clearance, adequate source control, oral tolerance, and azole-susceptible isolates, but this is often not feasible because of host- or pathogen-related factors [1, 5].
Rezafungin is a long-acting echinocandin with activity against multiple Candida species, including azole-resistant strains, and pharmacokinetic/pharmacodynamic (PK/PD) properties that allow once-weekly administration. Its prolonged half-life, high initial exposure, and broad tissue distribution make it an attractive option when treatment simplification or earlier discharge is desirable [3, 7, 9]. In randomized trials, rezafungin showed efficacy and safety comparable to caspofungin in candidemia and invasive candidiasis [7-9]. The approved regimen, 400 mg IV loading dose followed by 200 mg IV weekly, may also reduce infusion burden, vascular access manipulation, and potentially hospital stay in selected patients with appropriate follow-up [3, 9, 10].
Long-acting antimicrobials have been explored in other settings to facilitate discharge and reduce IV treatment burden, namely in selected Gram-positive bloodstream and catheter-related infections, but comparable strategies for invasive fungal infections are less established [11]. Shorter hospitalization and lower IV burden may also have sustainability advantages by reducing waste generation and greenhouse gas emissions [12-15].
The aim of our pilot study was to evaluate the feasibility, safety, and short-term outcomes of a stepwise antifungal strategy with rezafungin following initial short-acting echinocandin therapy in selected patients with catheter-related candidemia who were not suitable for oral azole step-down. We also explored its potential organizational and sustainability implications in a real-world setting.
METHODS
Study design
From January 1 to December 31, 2025, we conducted a prospective observational study in the medical wards of Pordenone and San Vito al Tagliamento Hospitals (a 400-bed hub and a 200-bed spoke, respectively) in Northeast Italy. These facilities serve approximately 320,000 residents and have a combined capacity of 150 medical ward beds. All catheter-related candidemia episodes, as defined by guidelines and microbiologic confirmation, were recorded through routine Infectious Diseases (ID) consultations as part of a structured antimicrobial stewardship (AMS) program.
Definitions
CRC was defined according to the 2009 Infectious Diseases Society of America (IDSA) guidelines as: (i) isolation of the same Candida species from simultaneous catheter-drawn (CD) and peripheral blood cultures (P-BCs), with CD-BC time-to-positivity at least two hours earlier; or (ii) isolation of the same Candida species from both the catheter tip and P-BCs [16].
Upon a yeast-positive blood-culture alert consistent with CRC, empirical IV echinocandin was started; the intravascular catheter was removed, and an ID evaluation (including imaging as indicated) was performed to rule out deep-seated infections.
Microbiological clearance was defined as the first negative blood culture with no subsequent positive blood cultures.
Clinical success at day 30 was defined as survival, resolution of candidemia-related signs and symptoms, no candidemia recurrence, and no further systemic antifungal therapy.
Estimated saved hospital days were calculated as the difference between the observed length of hospital stay after rezafungin administration and the 14-day inpatient course from the first persistently negative blood culture, for guideline-recommended echinocandin therapy, assuming continued daily inpatient administration.
Inclusion and exclusion criteria
Among screened CRC episodes, patients who met predefined stability criteria but were ineligible for oral azole step-down were transitioned to rezafungin and enrolled in our pilot study at that point.
Eligibility criteria included all of the following: hemodynamic stability; absence of fever for at least 48 hours; resolution of candidemia-related signs and symptoms; no other indication for inpatient care; documented candidemia clearance by blood culture; no echinocandin resistance; and unsuitability for oral fluconazole step-down (e.g., lack of oral route feasibility or adherence, contraindications or major interaction concerns, or non-susceptibility on antifungal susceptibility testing).
Exclusion criteria were pregnancy or breastfeeding; lack of informed consent from the patient or legal representative; identification of an alternative infectious focus or a different primary source of candidemia; eligibility for oral azole step-down.
Treatment protocol and toxicity monitoring
After initial echinocandin treatment, rezafungin was administered (single 400 mg IV dose) on day 7, provided blood culture clearance and predefined clinical eligibility criteria were satisfied. Patients were adequately informed about potential adverse events (e.g., electrolyte imbalances, gastrointestinal issues, and infusion-related reactions). Safety was monitored through clinical assessment and vital sign measurement during and after the infusion. At discharge, patients were instructed to contact the attending physician if any signs or symptoms suggestive of an adverse reaction. Any hospital readmission or unplanned contact was considered a potential adverse event related to drug administration.
Data collection and follow-up
Data were collected through patient interviews and electronic medical record review and included demographic characteristics, comorbidities (active malignancy, diabetes mellitus, immunosuppression, and chronic renal failure; KDIGO stage >3, age-adjusted Charlson Comorbidity Index). Additional data retrieved from hospital records included: type of intravascular device (short-term central venous catheter - CVC, peripherally inserted central catheter - PICC, or midline catheter), timing of clinical suspicion, timing of blood culture collection, initiation of empiric antifungal therapy, causative microorganism, antifungal susceptibility test results, drug-related adverse events, treatment discontinuation, and discharge date.
Follow-up at 30 and 90 days was conducted through outpatient assessment and/or structured telephone contact, complemented by review of electronic medical records.
Statistical analysis
Continuous variables were summarized as median (range), whereas categorical variables were summarized as count and percentage. Descriptive statistical analysis was performed using Microsoft Excel (Microsoft Corp., Redmond, WA, USA).
Outcomes
Primary outcomes were microbiological clearance and clinical success at day 30. Secondary outcomes included time to discharge after rezafungin administration, relapse, all-cause mortality at days 30 and 90, infection-related readmissions, and adverse drug events.
Microbiological assessment
Simultaneous blood cultures (BCs) were obtained from the catheter and from peripheral venipuncture in all enrolled patients. A single venipuncture was used to draw two BC sets. For each set, 8-10 mL of blood was collected in BACT/ALERT® FA Plus and BACT/ALERT® FN Plus bottles for the isolation of aerobic and anaerobic bacteria, respectively, and fungi. Incubation was performed in the automated BACT/ALERT VIRTUO® System bioMérieux, Italy and monitored for up to 5 days. Signal-positive bottles were processed for microscopic examination and for bacterial and/or fungal isolation on solid media. Upon Gram staining, microscopic observation of bacterial and/or fungal structures (blastospores and hyphal forms) was promptly communicated to the clinician.
Concurrently, culture on solid media was performed as follows: 1 µL of blood was inoculated onto Blood agar, MacConkey agar, Columbia CNA agar, and Sabouraud agar (VACUTEST KIMA S.r.l., Italy), then incubated at 37°C overnight for the isolation of aerobic bacteria and fungi; 1 µL of blood was inoculated onto Chocolate agar and Schaedler agar (VACUTEST KIMA S.r.l., Italia), then incubated at 37°C for 48 hours in CO2 and anaerobic atmospheres, respectively, for the isolation of fastidious and anaerobic bacteria. Identification of grown microorganisms was performed using Matrix-Assisted Laser Desorption Ionization Time-of-Flight Mass Spectrometry (MALDI-TOF MS) (VITEK-MS, BioMérieux, France).
Antimicrobial susceptibility testing for antifungals was performed using MICRONAUT 1640 media + MOPS + glucose (inkl. AST-Reagent Kit) in combination with the MICRONAUT-AM AFST plate (Bruker Daltonics GmbH and Co. KG, Germany), following the manufacturer’s instructions. After 24-72 hours of incubation at 35-37°C, the plates were visually read. Susceptibility to antifungal agents was evaluated for all fungal isolates according to EUCAST Clinical Breakpoints for fungi, version 11.0.
Follow-up blood cultures were collected every 48 hours until negative.
Ethical issues
Written informed consent for using routinely collected clinical data for clinical and research purposes was obtained from patients or their legal representatives at hospital admission. Data were de-identified after extraction and securely stored in compliance with Italian laws and regulations and the Declaration of Helsinki.
RESULTS
During the study period, 25 CRC episodes were identified overall across the two hospitals. Of these, 7 met all predefined clinical and microbiological criteria for rezafungin consolidation and were included in the present pilot cohort. All were female, with a median age of 74 years (range, 58–84) and a median age-adjusted Charlson Comorbidity Index of 7 (range, 3–10). Baseline characteristics, risk factors, management, and outcomes are summarized in Table 1.
Table 1 - Baseline characteristics, risk factors, management, and outcomes of the study cohort.
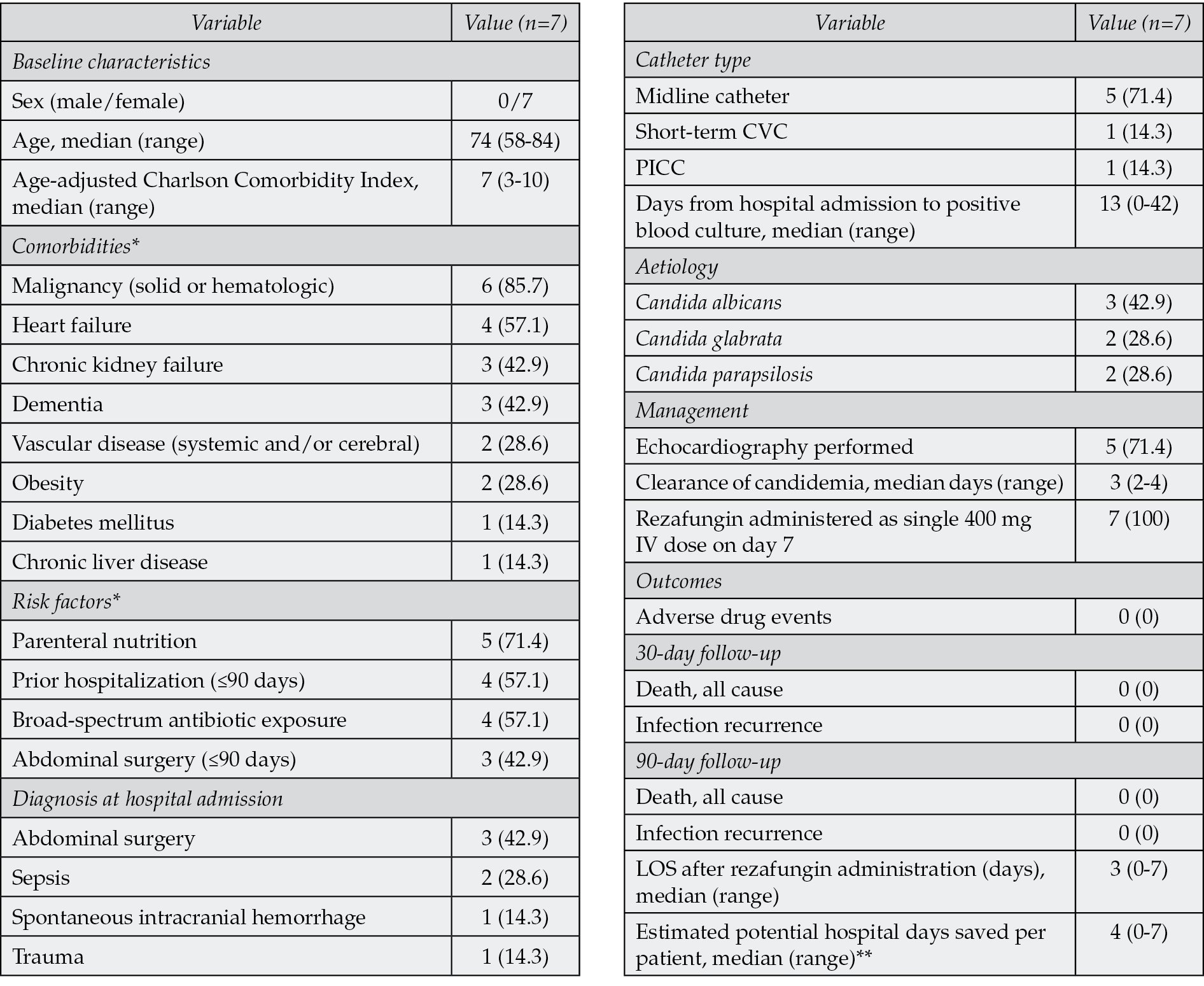
Notes: Data are n (%) unless otherwise indicated. Age, Charlson comorbidity index and days from hospital admission to first positive blood culture are expressed as median (range).
Abbreviations: CVC, central venous catheter; PICC, peripherally inserted central catheter; LOS, length of stay.
* Comorbidities and risk factors are not mutually exclusive.
** Estimated as the difference between the actual discharge date and the hypothetical date of completion of a 14-day inpatient course of daily intravenous echinocandin.
Clearance of candidemia indicates days from first positive blood culture to first documented negative blood culture. LOS after rezafungin administration indicates days from rezafungin administration to discharge.
The most common reason for hospitalization was abdominal surgery (3/7, 42.9%), followed by sepsis (2/7, 28.6%). One patient was admitted for intracranial hemorrhage, and one for trauma. Five patients (71.4%) received parenteral nutrition during hospitalization. Four (57.1%) had received broad-spectrum antibiotics in the preceding 90 days, four (57.1%) had been hospitalized within the 90 days, and three (42.9%) had undergone abdominal surgery in the 90 days before admission. Candidemia occurred a median of 13 days after admission (range, 0-42); one episode was detected on admission in a patient with an indwelling vascular catheter.
The causative organisms were Candida albicans in three cases (42.9%), Candida glabrata in two (28.6%), and Candida parapsilosis in two (28.6%). Five patients (71.4%) had a midline catheter, one had a PICC, and one had a short-term central venous catheter. Echocardiography was performed in five patients (71.4%). All patients received caspofungin at the time of candidemia alert (70 mg IV loading dose on day 0, followed by 50 mg IV once daily).
Blood culture clearance was achieved in all cases, with a median of 3 days (range, 2–4). After documented clearance and fulfilment of all predefined clinical criteria, rezafungin was administered on day 7 per protocol to all patients. Criteria for infeasibility of oral fluconazole step-down, including case-by-case microbiological and clinical factors, are detailed in Table 2. Clinical success at day 30 was achieved in all patients. No adverse events were recorded during or after rezafungin administration. No candidemia recurrences or deaths were observed at either 30- or 90-day follow-up. Based on the prespecified counterfactual, the median estimated number of hospital days saved per patient was 4 (range, 0-7), corresponding to 28 potential bed-days saved across the cohort.
Table 2 - Antifungal susceptibility and discharge timing for individual cases (n=7).
|
ID |
Candida Species |
Caspofungin MIC (mg/L) |
Fluconazole MIC (mg/L) |
Potential drug-drug interaction |
Catheter type |
Oral administration |
Discharge Day* |
|
1 |
C. albicans |
0.0625 |
1.0 |
- |
CVC |
Not feasible |
7 |
|
2 |
C. glabrata |
0.1250 |
4.0 |
- |
Midline |
Impaired (gastrectomy) |
4 |
|
3 |
C. parapsilosis |
0.5000 |
1.0 |
Warfarin |
Midline |
- |
5 |
|
4 |
C. glabrata |
0.1250 |
16.0 |
- |
PICC |
- |
1 |
|
5 |
C. albicans |
0.0600 |
0.3 |
Warfarin |
Midline |
- |
0 |
|
6 |
C. albicans |
0.1250 |
0.5 |
Warfarin |
Midline |
- |
3 |
|
7 |
C. parapsilosis |
0.2500 |
2.0 |
Escitalopram, Sotalol, Simvastatin |
Midline |
- |
1 |
Notes: Potential drug interaction indicates concomitant medications with clinically relevant interaction risk with oral azole therapy. Abbreviations: CVC, central venous catheter; PICC, peripherally inserted central venous catheter; MIC, minimum inhibitory concentration.
*=Days from rezafungin administration to discharge (day 0 = day of rezafungin dose).
DISCUSSION
This observational pilot study shows that a stepwise antifungal strategy, consisting of initial daily echinocandin therapy followed by rezafungin consolidation after clinical and microbiological stabilization, proved feasible, well tolerated, and associated with favorable short-term outcomes in a real-world cohort of CRC patients. Our findings align with prior analyses and emerging real-world experience demonstrating noninferior efficacy and comparable safety of rezafungin relative to caspofungin [7-9].
Although the small sample size precludes definitive conclusions, our cohort mirrors current candidemia epidemiology: elderly, multimorbid patients with healthcare exposure, similar to large European observational cohorts, that are often underrepresented in trials [1, 2]. Notably, no rezafungin-related adverse events occurred, despite the advanced age and comorbidities in our group.
This strategy was conceived as a consolidation approach for selected cases, preserving the core principles of candidemia management (early fungicidal therapy, source control, and microbiological response) when prolonged daily IV therapy would otherwise be necessary. This may occur in the presence of fluconazole–nonsusceptible species, such as C. glabrata, for which azole therapy may be suboptimal, or with elevated fluconazole MIC, or if fluconazole step-down is unsuitable due to patient-related factors, as shown in Table 2 [17-19]. Of note, two of our cases were caused by C. parapsilosis, a species for which echinocandin susceptibility may be less predictable. In our cohort, however, both isolates showed low caspofungin MIC values, and no microbiological failure or recurrence was observed. Rezafungin’s favorable PK/PD profile (high initial exposure, rapid attainment of therapeutic concentrations, and prolonged persistence above MIC) could enhance mycological clearance in these situations, as also suggested by recent pooled clinical data in C. parapsilosis candidaemia/invasive candidiasis [8, 20]. However, our sample is too small to support any species-specific conclusion.
Candidemia management is resource-intensive, particularly when patients remain hospitalized mainly to complete daily intravenous antifungal therapy [1, 2, 5]. Health-economic analyses consistently indicate that rezafungin can shorten hospital stays and reduce costs, a major driver of candidemia-related costs [21]. In our cohort, rezafungin consolidation therapy was associated with an estimated median reduction of 4 bed-days per patient (28 total bed-days saved), based on the prespecified counterfactual of a full inpatient echinocandin course. While a formal pharmacoeconomic analysis was beyond the scope of this study, applying published Italian per-day hospitalization estimates (€475.86/day for low-complexity hospitalization) yielded an exploratory estimate of approximately €1,903 per patient and €13,324 for the overall cohort, without accounting for antifungal acquisition costs [22].
Sustainability is also a concern, as each hospital bed-day generates significant waste, water use, and carbon emissions [14, 15]. Stewardship literature has increasingly framed long-acting agents as useful tools for reducing infusion burden, nursing workload, and single-use waste through targeted, high-value prescribing [21, 23]. For rezafungin specifically, although life-cycle assessment is lacking, extrapolated data from health-economic modeling suggest that shorter hospital stays may lower both economic costs and environmental impact [10, 12, 13, 19-23]. Our observed 4-day median reduction supports this potential benefit [8, 11].
This study has several limitations. Its pilot design, absence of a control group, and small sample size limit causal inference and generalizability. Moreover, patient selection was guided by clinical judgment, which may have introduced selection bias. Lastly, a formal pharmacoeconomic analysis was not performed; the cost estimates reported here are exploratory and based on a simplified counterfactual of avoided bed-days. Nevertheless, our findings offer preliminary real-world evidence supporting further research into long-acting antifungal agents to optimize candidemia care pathways.
In conclusion, our findings suggest that rezafungin appears safe and effective as part of a stepwise antifungal strategy for selected patients with candidemia, potentially enabling treatment simplification and earlier discharge. This approach promotes more patient-centered, sustainable care. Larger studies are needed to confirm these results and assess clinical, economic, and environmental outcomes.
Funding
No funding was received for this study.
Conflict of interest
No conflict of interest to be declared from the authors.
REFERENCES
[1] Soriano A, Honoré PM, Puerta-Alcalde P, et al. Invasive candidiasis: current clinical challenges and unmet needs in adult populations. J Antimicrob Chemother. 2023; 78(7): 1569-1585.
[2] Hoenigl M, Salmanton-García J, Egger M, et al. Guideline adherence and survival of patients with candidaemia in Europe: results from the ECMM Candida III multinational European observational cohort study. Lancet Infect Dis. 2023; 23(6): 751-761.
[3] Oliva A, De Rosa FG, Mikulska M, et al. Invasive Candida infection: epidemiology, clinical and therapeutic aspects of an evolving disease and the role of rezafungin. Expert Rev Anti Infect Ther. 2023; 21(9): 957-975.
[4] Tiseo G, Galfo V, Occhineri S, et al. Risk factors and outcomes of fungal superinfections in patients with severe COVID-19: an observational study from Pisa academic hospital. Infez Med. 2023; 31(1): 55-61.
[5] Cornely OA, Sprute R, Bassetti M, et al. Global guideline for the diagnosis and management of candidiasis: an initiative of the ECMM in cooperation with ISHAM and ASM. Lancet Infect Dis. 2025; 25(5): e280-e293.
[6] Moreal C, Angelini J, Venturini S, et al. Management of invasive fungal infection: clinical strategies in critical care from a multidisciplinary consensus. New Microbiol. 2025; 48(3): 211-214.
[7] Thompson GR 3rd, Soriano A, Honoré PM, et al. Efficacy and safety of rezafungin and caspofungin in candidaemia and invasive candidiasis: pooled data from two prospective randomised controlled trials. Lancet Infect Dis. 2024; 24(3): 319-328.
[8] Reinhold I, Mori G, Lanzafame M, et al. Rezafungin utilisation in real life - FungiScope results from Europe and the United States. Mycoses. 2025; 68(9): e70114.
[9] Thompson GR 3rd, Soriano A, Cornely OA, et al; ReSTORE trial investigators. Rezafungin versus caspofungin for treatment of candidaemia and invasive candidiasis (ReSTORE): a multicentre, double-blind, double-dummy, randomised phase 3 trial. Lancet. 2023; 401(10370): 49-59.
[10] Honoré PM, Bassetti M, Cornely OA, et al. Length of hospital and intensive care unit stay in patients with invasive candidiasis and/or candidemia treated with rezafungin: a pooled analysis of two randomised controlled trials. Crit Care. 2024; 28(1): 361.
[11] Venturini S, Reffo I, Avolio M, et al. Dalbavancin in catheter-related bloodstream infections: a pilot study. Infez Med. 2023; 31(2): 250-256.
[12] Ali S, Gash S, Weir N, et al. PO-llution control: a cross-sectional study on the role of antimicrobial stewardship in reducing healthcare’s carbon footprint. JAC Antimicrob Resist. 2025; 7(4): dlaf146.
[13] Weber DJ, Nori P, Ananthanarayanan R, Estelle C, et al. Society for Healthcare Epidemiology of America supports environmental stewardship and sustainability while protecting patients and healthcare personnel position statement of the SHEA Board. Antimicrob Steward Healthc Epidemiol. 2025; 6(1): e10.
[14] Prasad PA, Joshi D, Lighter J, et al. Environmental footprint of regular and intensive inpatient care in a large US hospital. Int J Life Cycle Assess. 2022; 27(1): 38-49.
[15] Zhang X, Albrecht K, Herget-Rosenthal S, Rogowski WH. Carbon footprinting for hospital care pathways based on routine diagnosis-related group (DRG) accounting data in Germany: An application to acute decompensated heart failure. J Ind Ecol. 2022; 26(4): 1528-1542.
[16] Mermel LA, Allon M, Bouza E, et al. Clinical practice guidelines for the diagnosis and management of intravascular catheter-related infection: 2009 Update by the Infectious Diseases Society of America. Clin Infect Dis. 2009; 49(1): 1-45.
[17] Wilson AG, Micek ST, Ritchie DJ. A retrospective evaluation of fluconazole for the treatment of Candida glabrata fungemia. Clinical Therapeutics. 2005; 27(8): 1228–1237.
[18] Yu DT, Peterson JF, Seger DL, Gerth WC, Bates DW. Frequency of potential azole drug-drug interactions and consequences of potential fluconazole drug interactions. Pharmacoepidemiol Drug Saf. 2005; 14(11): 755-767.
[19] Jeck J, Jakobs F, Kurte MS, Cornely OA, Kron F. Health-economic modelling of cost savings due to the use of rezafungin based on a German cost-of-illness study of candidiasis. JAC Antimicrob Resist. 2023; 5(3): dlad079.
[20] Soriano A, Locke JB, Cornely OA, et al. Clinical and mycological outcomes of candidaemia and/or invasive candidiasis by Candida spp. and antifungal susceptibility: pooled analyses of two randomized trials of rezafungin versus caspofungin. Clin Microbiol Infect. 2025; 31(2): 250-257.
[21] Di Gennaro F. Prescriptive appropriateness of dalbavancin in acute bacterial skin and skin structure infections in adults: an integrated approach between clinical profile, patient- and health system-related factors and focus on environmental impact. Front Antibiot. 2024; 3: 1405401.
[22] Foglia E, Ferrario L, Schettini F, et al. COVID-19 and hospital management costs: the Italian experience. BMC Health Services Research. 2022; 22: 991.
[23] Chakravorty AJ, Newman NJ, Veltri C, Spivak ES, Hecker MT, Hojat LS. Estimated carbon dioxide emissions associated with unnecessary intravenous antimicrobials administered in the hospital setting. Antimicrob Steward Healthc Epidemiol. 2025; 5(1): e263.