Le Infezioni in Medicina, n. 2, 205-219, 2026
doi: 10.53854/liim-3402-10
ORIGINAL ARTICLES
Epidemiology of imported malaria in an area of North-Eastern Italy (2016-2025): clinical focus on cerebral malaria
Lucia Corich1, Maria Teresa Bortolin1, Rosamaria Tedeschi1, Mariateresa Casarotto1, Antonella Pancino1, Alberto Molaro1, Valentina Anzanello1, Giancarlo Basaglia1, Maria Ada Corich2
1 Laboratory of Microbiology and Virology, Azienda Sanitaria Friuli Occidentale Santa Maria degli Angeli, Pordenone, Italy;
2 Department of Neurology, Azienda Sanitaria Friuli Occidentale Santa Maria degli Angeli, Pordenone, Italy.
Article received 3 February 2026 and accepted 24 March 2026
Corresponding author
Lucia Corich
E-mail: lucia.corich@asfo.sanita.fvg.it
SUMMARY
Background: In non-endemic settings, imported malaria poses diagnostic challenges due to non-specific presentations and lack of immunity, especially in visiting friends and relatives (VFRs). Focusing on the Western Friuli (Italy) observatory, this work aims to optimize triage by identifying early severity predictors. Through the analysis of clinical parameters, paediatric cerebral cases, and host genetics - including an illustrative case of HbS/β-thalassaemia - we evaluate the drivers of Plasmodium falciparum progression to improve patient management.
Methods: This retrospective study (2016–2025) analysed symptomatic malaria cases in the Friuli Occidentale Health Authority, combining epidemiological data with illustrative clinical cases. Diagnosis was confirmed via microscopy and molecular methods. Using WHO/AMCLI criteria, we evaluated admission parameters, including procalcitonin (PCT), C-reactive protein (CRP), and platelet count, to identify predictors of severe malaria, adopting a ≥2% parasitaemia threshold. Diagnostic accuracy was assessed via multivariable logistic regression and ROC analysis.
Results: Of the 124 malaria cases (P. falciparum 88.71%), 90.32% were VFRs, primarily from West Africa; only 12% reported adequate prophylaxis. Severe malaria occurred in 19.35% (24/124), including two cerebral malaria (CM) cases, with no fatalities. Severity fluctuated significantly, peaking at 60% (6/10; 95% CI 26.2%-87.8%) in 2025. Multivariable analysis identified parasitaemia ≥2% (aOR 8.44; 95% CI 2.41-29.58; p=0.001) and PCT (aOR 1.23; 95% CI 1.06-1.42; p=0.007) as the only independent severity predictors. PCT outperformed CRP (AUC 0.84 vs 0.73); at a 5.10 ng/mL cut-off, PCT demonstrated a 95.9% negative predictive value (NPV), effectively identifying low-risk patients. CM Case 1 (2017): A 5-year-old male with HbS/β-thalassaemia (VFR, from Ghana) admitted for P. falciparum malaria (9.5% parasitaemia) and severe anaemia, evolving into CM (loss of consciousness, seizures, BCS score 0); successfully treated with IV artesunate, antiepileptics, and blood transfusions, without sequelae. CM Case 2 (2022): A 3-year-old male (VFR, from Burkina Faso) with P. falciparum malaria (12.6% parasitaemia) evolving into CM (altered state of consciousness, EEG signs of cerebral distress, retinal haemorrhage, BCS score 2); resolved with IV artesunate and antiepileptics without sequelae.
Conclusions: Imported malaria remains a critical challenge due to unpredictable severity trends and non-specific onset of CM. PCT, combined with parasitaemia, outperformed CRP and platelet count as an independent predictor of severity. High PCT levels should serve as a “red flag” for immediate triage and parenteral therapy. Integrating PCT into clinical guidelines is essential for effective risk stratification and preventing life-threatening complications in non-endemic settings.
Keywords: imported malaria, epidemiology, visiting friends and relatives (VFRs), Plasmodium falciparum, cerebral malaria, sickle cell trait, biomarkers.
INTRODUCTION
Globally, malaria remains a leading cause of morbidity and mortality, particularly in low- and middle-income countries, where Plasmodium falciparum infection strains fragile healthcare infrastructures. In contrast, in non-endemic European settings, imported malaria presents a critical diagnostic and therapeutic challenge that differs fundamentally from the disease dynamics of endemic regions. While worldwide malaria mortality persists elevated, the issue in countries like Italy - officially malaria-free since 1970 - lies in managing a low-prevalence disease within a high-complexity healthcare system [1]. National surveillance systems often overlook the regional specificities, where shifting migratory patterns and international travel dynamics can rapidly alter the clinical landscape.
Predicting disease severity in such scenarios is clinically arduous. Unlike endemic regions where high pre-test probabilities and clinical experience guide triage, clinicians in non-endemic countries face considerable diagnostic uncertainty due to non-specific initial presentations that mimic common viral syndromes. Furthermore, the lack of protective immunity in travellers and visiting friends and relatives (VFRs) results in clinical courses that can rapidly escalate to severe forms, such as cerebral malaria (CM), which constitutes the most critical complication. Although in endemic areas CM predominantly affects children under 5 years of age due to immunological naivety and the vulnerability of the developing central nervous system (CNS), in non-endemic contexts it represents a severe threat to any individual lacking protective immunity [2, 3]. CM, primarily caused by P. falciparum, is defined as an acute, rapidly progressive febrile encephalopathy accompanied by an altered state of consciousness not attributable to other causes [4-6]. This condition presents a diagnostic dilemma due to its non-specific neurological onset; if not promptly treated, it carries a case-fatality rate approaching 100%, whereas with immediate and effective treatment, the rate decreases to 10-20% [2, 7-12].
Current literature lacks longitudinal and high-resolution data regarding epidemiological evolution within sub-regional European contexts. The Western Friuli area (North-Eastern Italy) fills this analytical gap as a relevant study setting due to its significant presence of settled migrant communities and VFR dynamics. Consequently, it serves as a strategic observatory for travel medicine and a sentinel point for monitoring clinical trends and diagnostic complexities in non-immune populations. Understanding the interplay between host genetics - exemplified by one case of HbS/β-thalassaemia compound heterozygosity in our cohort - and the clinical behavior of P. falciparum in this particular demographic is essential for improving patient triage and management. In such non-endemic environments, the interactions between host non-immunity and rapid parasitaemia dynamics are reflected in distinct biomarker kinetics that serve as early indicators of the risk of severe malaria outcomes. Based on this model, we hypothesize that defined clinical and laboratory parameters at admission can serve as reliable predictors of severe malaria, compensating for initial diagnostic uncertainty. This study aims to bridge the gap between surveillance and clinical practice by validating these predictors, with particular emphasis on the paediatric population and the early recognition of neurological complications. To evaluate these factors alongside the impact of host genetic variants, we analyzed the epidemiological and clinical landscape of imported malaria in Western Friuli over the 2016-2025 decade. By detailing the trajectories of two paediatric cases of CM, this work seeks to refine triage protocols and enhance overall public health preparedness.
MATERIALS AND METHODS
This retrospective observational study, incorporating an embedded series of illustrative clinical cases, examined all malaria diagnoses from January 2016 to December 2025 at the three facilities (one hub and two spoke hospitals) of the Friuli Occidentale Health Authority, serving approximately 310,000 residents in North-Eastern Italy. This dual design aims to clarify the epidemiological evolution while detailing specific clinical trajectories in high-risk patients. The primary outcome was the development of severe malaria during hospitalization, while secondary outcomes included the diagnostic accuracy of procalcitonin (PCT) and C-reactive protein (CRP) at presentation. The study population consisted of patients with symptomatic infection at the time of admission, characterized by fever or other malaria-related symptoms that prompted diagnostic evaluation. No asymptomatic cases were included in this cohort. For each patient, demographic data (date of birth, sex, country of malaria acquisition, and adherence to prophylaxis), and laboratory data (antigen and molecular results, species identification, parasitaemia index, haemoglobin (Hb), platelet count, total and direct bilirubin, blood glucose, creatinine, CRP, PCT, SpO2, and lactate) were collected. All laboratory and clinical data (including acidosis, CNS involvement, and co-infections) were retrospectively extracted from electronic medical records, having been originally obtained as part of standardized routine care at admission to evaluate their predictive value for early risk stratification.
Microbiological analysis was based on microscopic identification of P. falciparum, P. ovale, P. vivax, and P. malariae from Giemsa-stained thin and thick blood smears, following Plasmodium spp. detection via loop-mediated isothermal amplification (LAMP, Illumigene Malaria, Meridian Bioscience) and immunochromatographic antigen testing (Binax NOW Malaria, Abbott). Species identification was confirmed by Real-Time PCR (RealStar Malaria Screen & Type PCR kit 1.0, Altona Diagnostics). Commercial assays were performed according to the manufacturers’ instructions. For all P. falciparum positive samples, parasitaemia was calculated according to the guidelines of the Italian Association of Clinical Microbiologists (AMCLI) [13]. Only new diagnoses were included, excluding cases previously identified during the study period. Anaemia and thrombocytopenia were defined as Hb levels <11 g/dL and platelet count <150,000/µL, respectively. Anaemia was stratified as mild-to-moderate (Hb ≥7 g/dL) or severe (Hb <7 g/dL). Similarly, thrombocytopenia was classified as mild-to-moderate (30,000–150,000/µL) or severe (<30,000/µL).
Severe malaria was defined according to combined WHO and AMCLI criteria [2, 13]. Specifically, except for four endemic-area residents, a parasitaemia threshold ≥2% was adopted as a severity criterion for both non-immune Italian travellers (no prior exposure) and VFRs (with potentially waning semi-immunity), providing a rigorous rationale to avoid severity misclassification in a non-endemic context. CM was diagnosed in paediatric patients with P. falciparum parasitaemia and a Blantyre Coma Scale (BCS) score ≤ 2 persisting for >30 minutes after seizure control, according to WHO criteria and after excluding other causes of encephalopathy (e.g., hypoglycaemia or meningitis). Diagnosis was supported by clinical neurological assessment, and the exclusion of other encephalopathies through brain Computed Tomography (CT) scans, when clinically indicated.
Ethical considerations
This study adhered to the Declaration of Helsinki. In accordance with national and Italian Data Protection Authority guidelines, formal Institutional Review Board approval and informed consent were waived due to the retrospective use of fully anonymized routine clinical data.
Statistical analysis
Categorical variables were expressed as percentages and continuous variables as means ± standard deviations (SD). Comparisons were performed using Student’s t-test. Independent predictors of severe malaria were identified via multivariable logistic regression, adjusting for age, immune status (VFR vs. others), diagnostic delay (days from symptom onset to admission), Plasmodium species (P. falciparum vs. others), parasitaemia (≥ 2%), PCT, and CRP. Continuous markers (PCT, CRP) were dichotomized based on optimal cut-offs. Adjusted Odds Ratios (aOR) with 95% confidence intervals (CI) were calculated. A complete-case analysis was applied for missing data (e.g., prophylaxis), with sensitivity analyses confirming no significant bias. Diagnostic accuracy was assessed through receiver operating characteristic (ROC) curves and the area under the curve (AUC); optimal cut-offs were determined using the Youden Index (J), with subsequent calculation of sensitivity, specificity, and negative predictive value (NPV). Temporal trends in severity were reported as proportions with 95% CI (Clopper-Pearson method). Significance was set at p< 0.05. Analyses were performed using Python (v. 3.10) and MedCalc (v. 22.0).
RESULTS
Epidemiological Characteristics
During the decade under review, 129 malaria diagnoses were performed; the analysis included 124 cases, following the exclusion of 5 P. falciparum reinfections. Of the 124 new episodes: 110 (88.71%) were caused by P. falciparum, 6 (4.84%) by P. ovale, 4 (3.23%) by P. vivax, 3 (2.42%) by P. malariae, and 1 (0.81%) by a mixed infection with P. falciparum and P. malariae (Figure 1). The majority of patients were male (73%), and belonged to the 18-65 age group (75%) (Figure 2). Regarding patient categories, 90.32% were VFRs; 1.61% were Italian returning from endemic countries for business trips, and 4.03% for tourism; 2.42% were Italian residents in endemic countries returning to Italy for work, travel, or family visits, and 1.61% were individuals from endemic countries who had arrived in Italy a few days earlier. The infection was primarily contracted in West Africa, with the highest number of cases (55%) occurring in Burkina Faso (Figure 3). Non-malarial co-infections were observed in only 4 patients: 1 case of concurrent Adenovirus and 1 case of Rhinovirus detected via nasopharyngeal swab, 1 case of Salmonella sp. isolated from stool culture, and 1 case of Escherichia coli from urine culture.
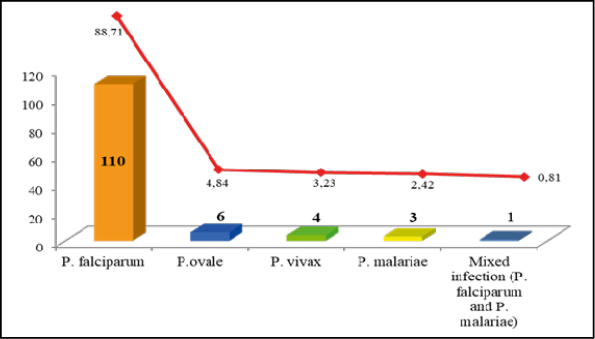
Figure 1 - Distribution of malaria cases by species (2016–2025). The red line indicates the percentage for each species.
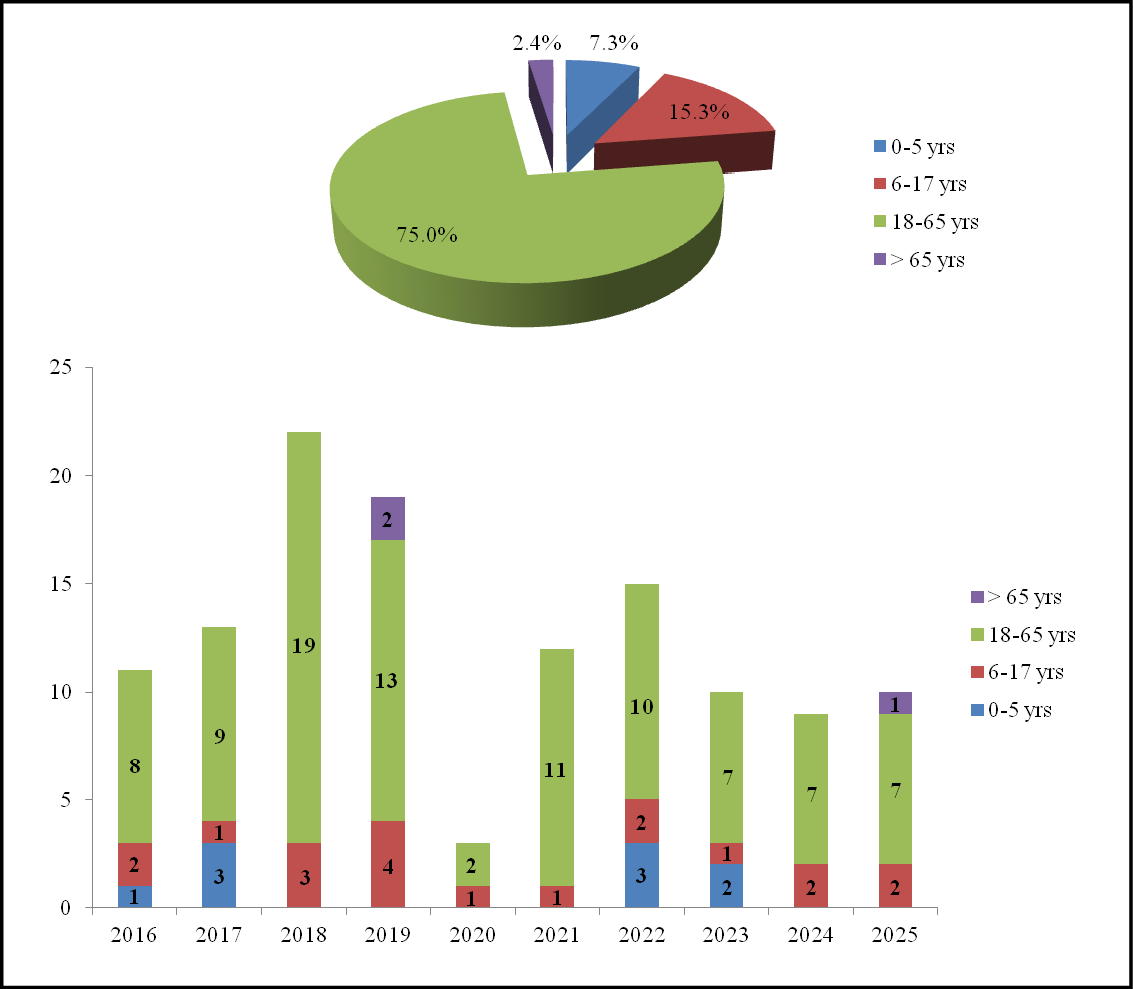
Figure 2 - Distribution of malaria cases by age group: percentage (upper) and annual absolute numbers (lower).
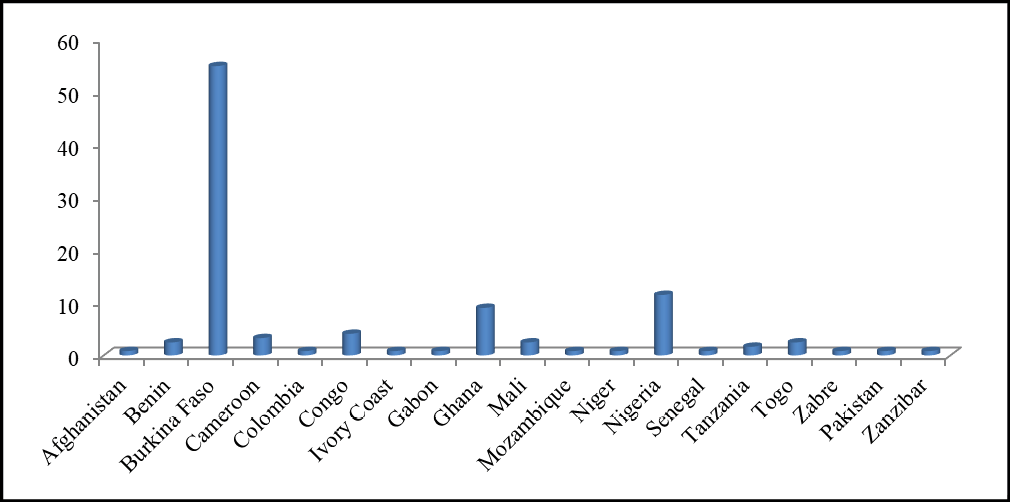
Figure 3 - Percentage of malaria cases by country of acquisition (2016–2025).
The case trend varied over the decade. A peak was recorded in 2018 (22 cases), followed by a predictable and significant reduction during the first year of the COVID-19 pandemic (2020), a recovery in the following two years, and finally, a stabilisation at lower levels compared to the pre-pandemic period (Figure 4).
Concerning chemoprophylaxis (missing data for 41 episodes, 33%), only 12% of patients reported adequate adherence, while 29% used no pharmacological prevention and 26% showed partial adherence.
Of the 124 diagnoses, 24 (19.35%) were classified as severe malaria, 7 of which involved children between 2 and 5 years of age. The distribution of severe forms was highly variable, ranging from 0% in 2020 (0/3; 95% CI 0.0% - 70.8%) and 2024 (0/9; 95% CI 0.0% - 33.6%) to a peak of 60% in 2025 (6/10; 95% CI 26.2% - 87.8%) (Figure 5). The annual trend of the absolute number of malaria cases, distinguishing between severe and uncomplicated forms, is illustrated in Figure 6 and detailed in Table 1. Among the patients with severe malaria, 22 were VFRs and 2 were Italian travellers returning from endemic areas. In patients with severe malaria, the prophylaxis profile was as follows: complete adherence in 29% of cases, partial in 29%, absent in 25%, and unavailable for 17%. No deaths occurred.
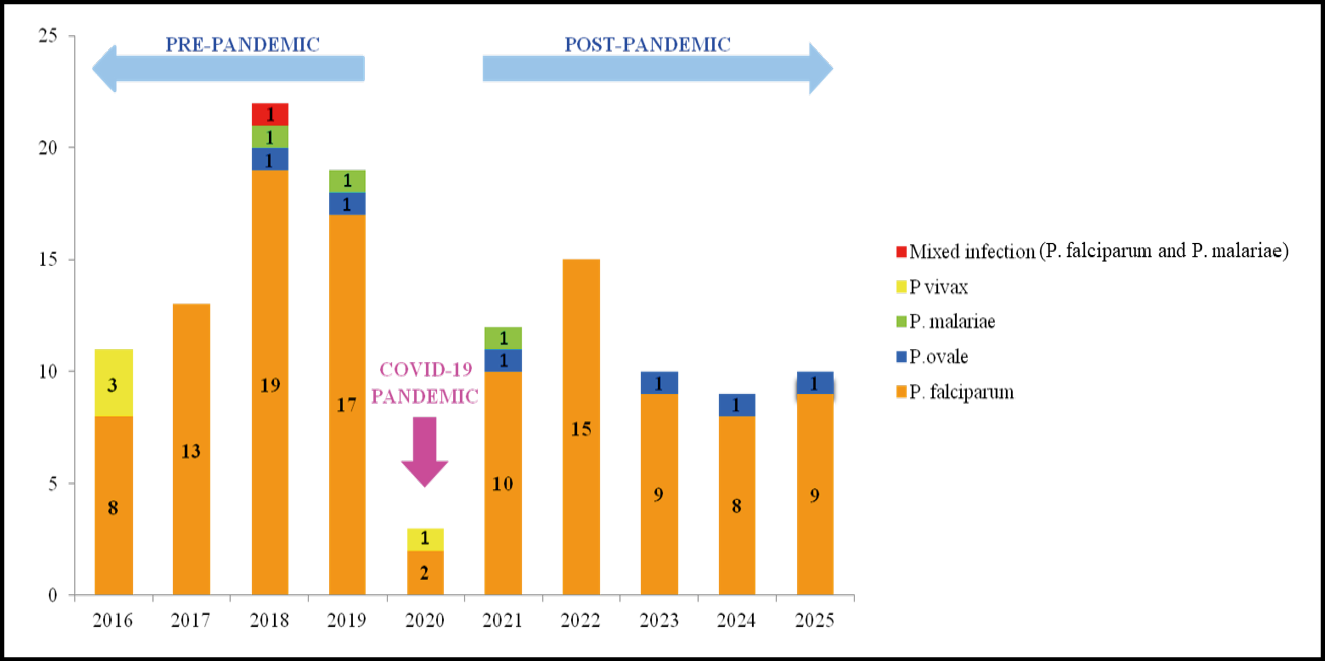
Figure 4 - Absolute number of malaria cases by species and year.
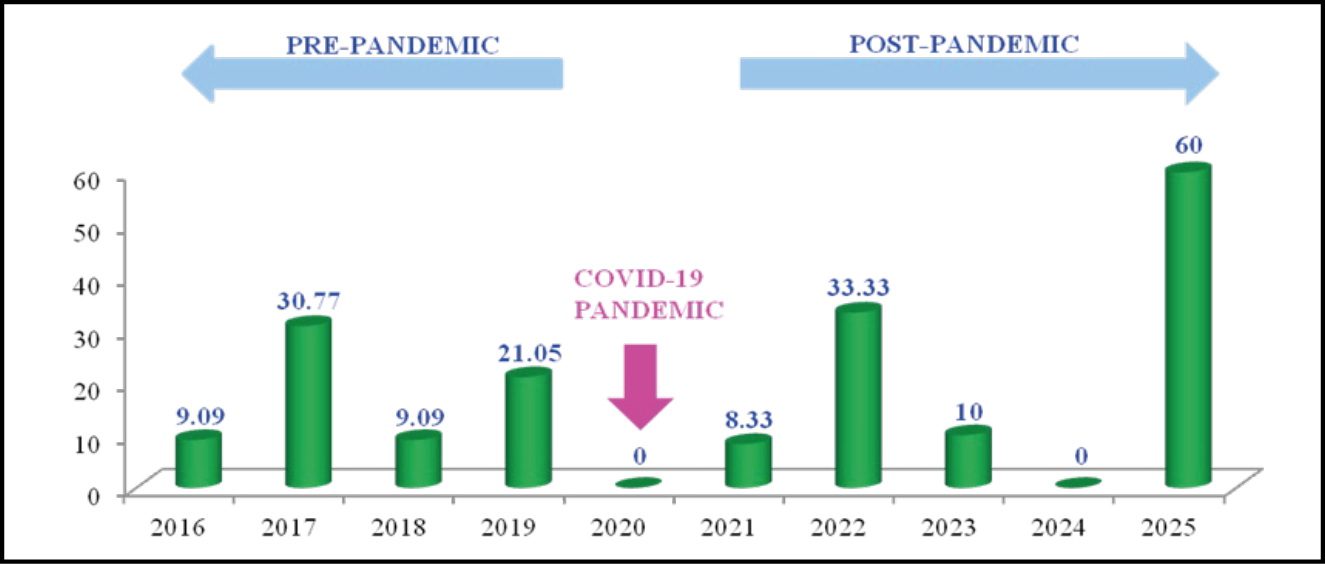
Figure 5 - Annual percentage of severe malaria cases: pre-, during, and post-COVID-19 pandemic.
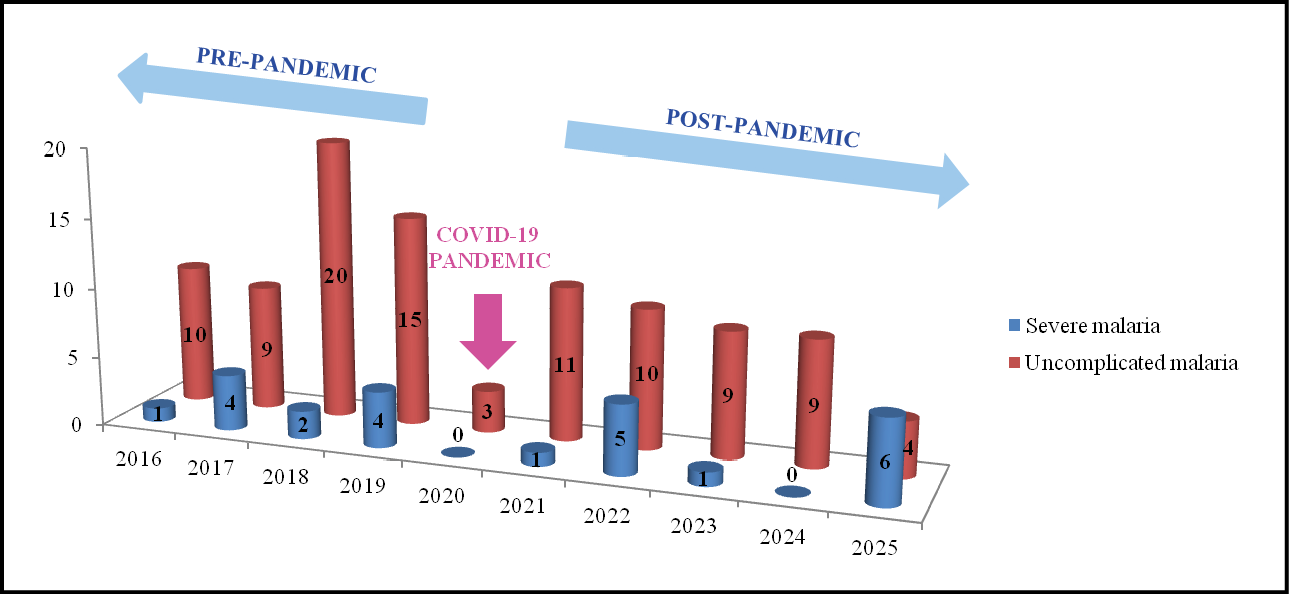
Figure 6 - Annual comparison of absolute numbers: severe vs. uncomplicated malaria, pre-, during, and post-COVID-19 pandemic.
Table 1 - Temporal Trends of severe and uncomplicated malaria (2016-2025).
|
Year |
Absolute number |
Severe Malaria, n (%) |
95% |
Uncomplicated Malaria |
95% |
|
2016 |
11 |
1 (9.1%) |
0.2% – 41.3% |
10 (90.9%) |
58.7% – 99.8% |
|
2017 |
13 |
4 (30.8%) |
9.1% – 61.4% |
9 (69.2%) |
38.6% – 90.9% |
|
2018 |
22 |
2 (9.1%) |
1.1% – 29.2% |
20 (90.9%) |
70.8% – 98.9% |
|
2019 |
19 |
4 (21.1%) |
6.1% – 45.6% |
15 (78.9%) |
54.4% – 93.9% |
|
2020 |
3 |
0 (0.0%) |
0.0% – 70.8% |
3 (100.0%) |
29.2% – 100.0% |
|
2021 |
12 |
1 (8.3%) |
0.2% – 38.5% |
11 (91.7%) |
61.5% – 99.8% |
|
2022 |
15 |
5 (33.3%) |
11.8% – 61.6% |
10 (66.7%) |
38.4% – 88.2% |
|
2023 |
10 |
1 (10.0%) |
0.3% – 44.5% |
9 (90.0%) |
55.5% – 99.7% |
|
2024 |
9 |
0 (0.0%) |
0.0% – 33.6% |
9 (100.0%) |
66.4% – 100.0% |
|
2025 |
10 |
6 (60.0%) |
26.2% – 87.8% |
4 (40.0%) |
12.2% – 73.8% |
Note: 95% Confidence Intervals (CI) were calculated using the Clopper-Pearson exact method. Percentages are calculated on the total number of malaria cases diagnosed per year.
Laboratory and Clinical Features
Of the 24 severe malaria cases, 23 were caused by P. falciparum and 1 by P. ovale. Severe thrombocytopenia (<30 x 103 platelets/µL) was found in 4 patients, and mild-to-moderate thrombocytopenia (30-150 x 103 platelets/µL) in 72. Severe anaemia (Hb <7 g/dL) was observed in 3 patients, while 20 presented with mild-to-moderate anaemia (Hb 7-11 g/dL) (Table 2). Notably, no patient presented with concurrent severe thrombocytopenia and severe anaemia.
Patients with severe malaria showed significantly higher PCT levels compared to uncomplicated cases (p= 0.016), as well as higher CRP levels (p= 0.039). Conversely, no significant difference was observed in platelet count (p= 0.37).
Table 2 - Laboratory findings of imported malaria cases.
|
Laboratory parameters |
Blood values |
|
Plateletsa, mean (x103/µL ± SD) |
125 ± 80.87 |
|
Thrombocytopenia, n (%) |
76 (68.47) |
|
Severe (<30,000 platelets/µL) |
4 (3.60) |
|
Mild-to-moderate |
72 (64.86) |
|
Haemoglobinb, mean (g/dL ± SD) |
12.53 ± 2.50 |
|
Anaemia, n (%) |
23 (20.54) |
|
Severe (<7 g/dL) |
3 (2.68) |
|
Mild-to-moderate (7-11 g/dL) |
20 (17.86) |
|
Parasitaemiac, n (%) |
|
|
<2% |
85 (78.70) |
|
2-5% |
14d (12.96) |
|
>5% |
9 (8.33) |
Notes:
n = number of patients.
a Data were available for 111 patients.
b Data were available for 112 patients.
C Calculated for P. falciparum (critical threshold ≥2%).
d Four patients were potentially semi-immune.
To further investigate these findings and isolate the independent drivers of severity, a multivariable logistic regression model was performed, incorporating age, immune status, diagnostic delay, Plasmodium species, and inflammatory markers. While CRP was associated with severity in the univariate analysis, the multivariable model confirmed that only a parasitaemia threshold ≥2% (aOR 8.44; 95% CI 2.41-29.58; p=0.001) and PCT levels (aOR 1.23; 95% CI 1.06–1.42; p=0.007) remained independent predictors of severe malaria (Table 3). Following adjustment, CRP lost significance (p=0.485), suggesting its elevation was likely secondary to other factors rather than an independent predictor. No significant independent association was found for diagnostic delay or age. To further refine triage decision-making, we calculated clinical performance metrics for both biomarkers. PCT demonstrated superior diagnostic accuracy compared to CRP, with an AUC of 0.84 (95% CI 0.74-0.94) versus 0.73 (95% CI 0.61–0.85), respectively. Using an optimal cut-off of >5.10 ng/mL, PCT achieved a sensitivity of 84.6% and a specificity of 78.3%. Importantly, the NPV for PCT was 95.9%, indicating that levels below this threshold effectively identify patients at low risk of severe complications. In contrast, CRP at its optimal cut-off (>12.0 mg/dL) showed lower sensitivity (72.2%) and NPV (93.2%).
Table 3 - Multivariable logistic regression analysis of predictors for severe malaria (n= 124).
|
Variable |
aOR |
95% CI |
p-value |
|
Parasitaemia ≥ 2% |
8.44 |
2.41 – 29.58 |
0.001 |
|
PCT |
1.23 |
1.06 – 1.42 |
0.007 |
|
CRP |
1.01 |
0.99 – 1.03 |
0.485 |
|
Age |
1.04 |
0.99 – 1.09 |
0.165 |
|
VFR status (vs. other travellers) |
0.72 |
0.21 – 2.51 |
0.605 |
|
Diagnostic delay (days) |
1.06 |
0.89 – 1.25 |
0.542 |
|
P. falciparum (vs. others) |
1.58 |
0.39 – 6.42 |
0.518 |
Notes: aOR, adjusted Odds Ratio; CI, confidence interval; PCT, procalcitonin; CRP, C-reactive protein; VFR, visiting friends and relatives.
The multivariable model was adjusted for all variables listed in the table: parasitaemia ≥2%, PCT, CRP, age, immune status (VFR vs. non-immune), diagnostic delay (number of days from symptom onset to hospital admission), and Plasmodium species.
Bold p-values indicate statistical significance (p<0.05). An aOR >1 indicates an increased risk of severe malaria, while a 95% CI not including 1.00 confirms the statistical significance of the association.
P. falciparum hyperparasitaemia was identified in 19 patients. However, 4 residents of endemic areas with parasitaemia between 2% and 5% were excluded from this count, given their likely semi-immunity (Table 2). One patient reached a peak parasitaemia of 27%, while in another case, an extremely low parasitaemia (0.06%) was detected, a value potentially influenced by concomitant severe anaemia (Hb 1.7 g/dL). Regarding other severity criteria: 1 patient was classified as having severe malaria based on laboratory parameters (total bilirubin >3 mg/dL with 4.5% parasitaemia), 1 due to acute renal failure (creatinine 3.5 mg/dL), and 2 due to haemoglobinuria, one of which occurred in the only severe malaria episode caused by a non-falciparum species (P. ovale). Finally, two patients progressed to CM.
First Case of CM
The first case dates back to 2017 and concerns a 5-year-and-6-day-old male (second-generation VFR), affected by HbS/β-thalassaemia compound heterozygosity. He had returned the day before from Ghana, where he had stayed for 1 month and 11 days without completing the antimalarial prophylaxis course. The child had already been to Ghana three years earlier. His medical history was negative for previous malaria episodes, but included numerous Emergency Department visits and hospitalizations for acute pain involving the bones, abdomen, and chest due to vaso-occlusive crises often associated with fever, vomiting, rhinorrhea, and cough; no prior febrile seizures were reported. He was on prophylactic antibiotic therapy with amoxicillin (5 mL twice daily). A few days before leaving for Ghana, he had been hospitalized for a painful crisis and right-sided pneumonia. At discharge, his Hb level was 7.8 g/dL.
The patient presented to the Emergency Department due to jaundice that had been worsening for one week, loss of appetite, cough, and an episode of vomiting.
Upon physical examination, he was in fair general condition, oppositional during the assessment. Clinical findings included icteric sclerae and dark skin with a jaundiced tint. Oral mucosae were pale, and the tongue was coated. He was tachycardic (135 bpm) with a low-grade fever (37.6°C) and hypotensive (86/37 mmHg); a 2/6 mid-systolic murmur was noted. Breath sounds were slightly harsh, with good air entry and no frank adventitious sounds (SpO2 96% on room air). The abdomen was soft and non-tender, with the spleen palpable 1 cm below the costal margin and the liver 3-4 cm below the right costal margin. Tympanic membranes were intact, no neck stiffness was noted, and his weight was 19.2 kg. The child was admitted to the Paediatric ward.
Admission blood tests (Table 4) revealed severe anaemia, marked inflammation, early dehydration, tissue hypoxia, and hepatic impairment. Microscopic observation of thin and thick blood smears confirmed P. falciparum infection with 9.5% parasitaemia. Blood cultures were negative. Management began with intravenous (IV) rehydration (saline-glucose solution), a packed red blood cell (pRBC) transfusion, and IV quinine (20 mg/kg over 4 hours) under cardiac and glucose monitoring, without side effects. Subsequently, albumin (1 g/kg) was administered, and fluid balance and urine output monitoring were initiated. A chest ultrasound showed a small right mid-apical consolidation, multiple B-lines, and bilateral pleural effusion (<1 cm). IV antibiotic coverage was started (amoxicillin + clavulanic acid, 30 mg/kg per dose every 8 hours). By the following morning, parasitaemia had decreased to 3%, while Hb rose to 7.3 g/dL; IV artesunate was then initiated (3 doses at 12-hour intervals).
Table 4 - Blood test results of the first patient on admission to the Emergency Department.
|
Laboratory parameters |
Blood values |
Reference intervals |
|
Leukocytes |
18.88 x 103/µL |
5.50 - 15.50 |
|
Haemoglobin |
4.0 g/dL |
11.5 - 13.5 |
|
Hematocrit |
11.20% |
34.0 - 40.0 |
|
Platelets |
351 x 103/µL |
140 - 440 |
|
Sodium |
134 mmol/L |
135-145 |
|
Potassium |
Hemolysed sample |
3.5 - 5.0 |
|
Chloride |
102 mmol/L |
97 - 110 |
|
Glucose |
115 mg/dL |
|
|
Creatinine |
0.60 mg/dL |
0.20 - 1.20 |
|
ALT |
151 U/L |
6.0 - 78 |
|
Total Bilirubin |
29.4 mg/dL |
0.2 - 1.2 |
|
Direct Bilirubin |
0.3 mg/dL |
0.0 - 0.4 |
|
LDH |
Hemolysed sample |
100 - 240 |
|
Lactic Acid |
4.57 mmol/L |
0.9 - 2.0 |
|
C-reactive protein |
8.4 mg/dL |
0.0 - 0.5 |
|
Procalcitonin |
10.76 µg/L |
0.02 - 0.05 |
|
pH (venous blood |
7.35 |
7.32-7.42 |
In the afternoon, the patient’s condition deteriorated rapidly with tachypnea (up to 70 bpm) and tachycardia (up to 210 bpm), though oxygen saturation remained stable. During a high-grade fever (up to 42°C) unresponsive to antipyretics, he experienced an episode of generalized rigidity, loss of consciousness, and head/eye deviation with meningism (BCS score 0). The episode lasted over 5 minutes and resolved following administration of IV diazepam. Upon regaining consciousness, the child exhibited agitation and delirium, which resolved after administration of IV midazolam. The temperature only decreased following oral administration of metamizole.
In the subsequent hours, clinical improvement was observed, with the patient resuming self-feeding and reactivity. He exhibited persistent coughing fits and a markedly distended abdomen due to meteorism and hepatosplenomegalia (confirmed by ultrasound), in the absence of ascites. The next day, due to a further drop in haemoglobin, a second unit of pRBCs was transfused. The fundoscopic exam was negative. The cardiological evaluation revealed a mild pericardial effusion without hemodynamic significance, probably secondary to the infectious process. Artesunate therapy was subsequently transitioned to oral dihydroartemisinin/piperaquine for an additional 3 doses, with daily parasitaemia monitoring. Parasitaemia cleared by the final day of antimalarial treatment. Jaundice progressively improved with a decrease in bilirubin levels. Subsequent follow-up visits showed no further abnormalities.
Second Case of CM
The second case occurred in 2022 and involved a 3-year-and-6-month-old male (second-generation VFR). He had returned 5 days earlier from his first trip to Africa (Burkina Faso), which lasted 2 months and 11 days, for which he had taken malaria prophylaxis with mefloquine (Lariam) fairly regularly. He had been febrile for two days and, on the day of admission to the Emergency Department, also presented with abdominal pain; no diarrhea or vomiting were reported. The patient was admitted to the Paediatric ward. Upon presentation, he was alert, oriented, and eupneic, with rhythmic cardiac activity. Vital signs were as follows: temperature 38°C, heart rate 114 bpm, blood pressure 78/65 mmHg, and SpO2 97% on room air; his weight was 16 kg. The abdomen was painful and slightly tense, making the liver and spleen difficult to palpate; urine output was adequate. No jaundice, seizures, or motor deficits were observed. Pharyngeal and tympanic membrane examinations were unremarkable.
Laboratory tests (Table 5) revealed mild anaemia, thrombocytopenia, hyponatraemia, and elevated markers of hepatic cytolysis, cholestasis, and systemic inflammation. Urinalysis was negative for leukocytes and bacteria; a third-generation COVID-19 antigen swab was negative. Blood cultures were also negative. Parasitaemia was 12.6%. The electrocardiogram showed no abnormalities. Treatment was initiated with IV artesunate (2 doses 12 hours apart), IV amoxicillin-clavulanic acid, and rehydration with 0.9% saline and 5% glucose. Fever persisted, responding only temporarily to oral antipyretics.
Table 5 - Blood test results of the second patient on admission to the Emergency Department.
|
Laboratory parameters |
Blood values |
Reference intervals |
|
Leukocytes |
9.87 x 103/µL |
5.50 - 15.50 |
|
Haemoglobin |
10.5 g/dL |
11.5 - 13.5 |
|
Hematocrit |
31.10% |
34.0 - 40.0 |
|
Platelets |
72 x 103/µL |
140 - 440 |
|
Sodium |
132 mmol/L |
135-145 |
|
Potassium |
4.4 mmol/L |
3.5 - 5.0 |
|
Chloride |
96 mmol/L |
98 - 109 |
|
Glucose |
75 mg/dL |
|
|
Creatinine |
0.42 mg/dL |
0.20 - 1.20 |
|
ALT |
152 U/L |
6.0 - 78 |
|
AST |
280 U/L |
3.0 - 40 |
|
Total Bilirubin |
3.0 mg/dL |
0.2 - 1.2 |
|
Direct Bilirubin |
1.0 mg/dL |
0.0 - 0.4 |
|
LDH |
597 U/L |
90 - 240 |
|
C-reactive protein |
13.9 mg/dL |
0.0 - 0.5 |
|
Procalcitonin |
7.89 µg/L |
0.02 - 0.05 |
|
pH (venous blood |
7.33 |
7.32-7.42 |
On the second day, the patient developed trismus with altered consciousness and fixed pupils; he was responsive only to painful stimuli and presented with staring eyes (BCS score 2), in the absence of respiratory distress (SpO2 >98%, blood pressure 97/76 mmHg, blood glucose 84 mg/dL). Brain CT scan showed no significant abnormalities. Fundoscopic examination revealed retinal haemorrhage. An initial recovery of the pupillary light reflex was observed; however, after 30 minutes, trismus and upper limb rigidity recurred, requiring the administration of 10 mg of rectal diazepam, which provided relief.
The patient remained lethargic, maintaining SpO2 98% on room air and blood pressure 97/76 mmHg; body temperature was 37.1°C. He was transferred to the Paediatric Intensive Care Unit (ICU) at the Burlo Garofalo Specialized Paediatric Hospital in Trieste (Italy) due to severe P. falciparum malaria (12% parasitaemia and hyperbilirubinaemia) complicated by neurological manifestations, including altered sensorium and suspected recurrent focal seizures. During his ICU stay, the child began antiepileptic therapy with levetiracetam after an electroencephalogram (EEG) showed signs compatible with cerebral distress. IV artesunate was continued and subsequently shifted to oral therapy with dihydroartemisinin/piperaquine (320/40 mg), which was suspended once parasitaemia cleared.
No further seizures occurred, and the EEG pattern progressively improved. Ten days after admission, the child was discharged on levetiracetam therapy. Follow-up visits showed no abnormalities, and the antiepileptic therapy was gradually tapered.
DISCUSSION
The temporal distribution of malaria episodes varied during the 2016–2025, peaking in 2018 (17.6%). Case numbers pre- and post-COVID-19 pandemic appeared almost symmetrical, although they remained lower in recent years. The pandemic-related reduction was likely multifactorial, driven by stringent travel restrictions, limited healthcare access, and potential underdiagnosis due to symptom overlap with SARS-CoV-2.
Most infections (88.71%) were caused by P. falciparum among VFRs returning from West Africa, particularly Burkina Faso. This pattern reflects high regional endemicity of the parasite and poor chemoprophylaxis adherence due to risk misperception among these travellers. Furthermore, it confirms that childhood-acquired immunity wanes after years of residence in malaria-free areas, leaving VFRs susceptible to severe disease upon their return to endemic regions [14]. Our data (available for 67% of patients) show improved prophylaxis awareness compared to the previous decade; however, the high treatment interruption rate suggests the need for better education on complete adherence [15].
Severe presentations varied throughout the decade, being recorded in all but two years. Remarkably, after a total absence in 2024, a surge occurred in 2025, including the study’s highest parasitaemia (27%). This unpredictable spike warrants vigilance and likely results from a combination of factors: waning immunity, delayed diagnosis due to late health-seeking behavior, potential spread of drug-resistant P. falciparum strains in West Africa, and shifting travel patterns, such as longer stays in endemic regions. Analysis of PCT and CRP concentrations revealed significantly higher levels in severe cases aligning with previous reports [16, 17]. However, our multivariable model refined this observation, identifying only PCT as a significant independent predictor of severity in our cohort. While CRP is a sensitive but non-specific indicator of inflammation, its loss of significance after adjustment suggests that its elevation in severe cases is likely a secondary reflection of the overall parasite burden and systemic response. In contrast, PCT offers a more robust and independent signal of clinical deterioration. Furthermore, platelet count showed no significant differences between the two groups, reflecting the ongoing debate regarding its prognostic value [18, 19]. In summary, although CRP and thrombocytopenia are frequent in malaria, they act as general infection markers rather than specific severity predictors. Conversely, PCT achieved a robust AUC (0.84), reinforcing its role as the sole independent predictor in our multivariable model. Clinically, PCT and CRP offer rapid turnaround times (< 2 hours); however, while CRP is more cost-effective, it remains a suboptimal severity predictor. In contrast, the superior predictive value of PCT justifies its use to expedite high-risk patient care, especially when initial parasitaemia is low. These findings concord with previous Italian and European cohorts – including France, the Netherlands and Germany - where PCT demonstrated high diagnostic accuracy for severe malaria [20-24]. Such consistency supports the generalizability of PCT as a reliable tool for non-immune patients in non-endemic contexts. Nevertheless, these results represent strong associations that warrant further confirmation in larger, prospectively validated cohorts.
The most relevant metric for triage is the NPV (95.9% at 5.10 ng/mL), suggesting PCT could effectively identify low-risk patients, streamlining Emergency Department decisions and prioritizing resources for those requiring aggressive management. This is vital in European acute-care settings, where managing imported malaria in non-immune travellers is recurrent and early risk stratification is crucial to prevent rapid clinical deterioration. Integrating PCT into diagnostic protocols would enable more structured pathways, facilitating prompt identification of high-risk individuals while avoiding unnecessary ICU admissions for low-risk cases.
It is well established that severe malaria is predominantly caused by P. falciparum, which can lead to multi-organ complications. The severity of P. falciparum infection is driven by PfEMP1-mediated cytoadherence and “rosetting”, which causes microvascular obstruction, particularly in the brain [25]. Such sequestration impairs microcirculation and triggers cytokine release responsible for symptoms. This mechanism, controlled by var genes, allows the parasite to evade host immune responses through continuous antigenic variation [25-27].
Clinically, these processes lead to manifestations defined by established criteria for severe malaria, including high P. falciparum parasitaemia, acidosis, severe anaemia, shock, pulmonary oedema, acute respiratory distress syndrome, acute kidney injury, abnormal bleeding, disseminated intravascular coagulation, or neurological involvement such as altered consciousness and seizures, which significantly increase mortality risk, as seen in CM [28].
In our cohort of 24 severe malaria cases, hyperparasitaemia was the primary severity marker, often complicated by severe anaemia, renal failure, and haemoglobinuria. Notably, two patients progressed to CM. Both - one of whom had HbS/β-thalassaemia compound heterozygosity - presented to the Emergency Department with non-specific symptoms: jaundice and low-grade fever in the first patient, and fever and abdominal pain in the second. In line with previous studies, this observation underscores that mild initial symptoms cannot rule out CM [8, 29-31]. Our patients developed neurological signs, specifically epileptic seizures, after admission. While common in children, such seizures in severe malaria should be considered indicators of direct cerebral involvement rather than mere febrile seizures [6, 32]. Neurological dysfunction and seizures are in fact attributable to hypoxic damage induced by the sequestration of parasitized cells in the cerebral microcirculation, as well as to direct axonal injury caused by malarial pigments and neurotoxic cytokine release [5]. Importantly, neither patient presented with hypoglycaemia or acidosis, which are frequent in paediatric CM [33]. Low blood glucose at admission is among the earliest prognostic biomarkers identified in paediatric malaria [8]. Many clinical models for assessing the risk of severe malaria, neurological sequelae, and mortality include hypoglycaemia (typically < 2.2 mmol/L or < 40 mg/dL) as a key predictive parameter [34, 35]. Our patients maintained stable glucose levels throughout their hospitalization; while this aligns with their favorable outcomes, it emphasizes that severe malaria does not invariably present with hypoglycaemia, highlighting the clinical heterogeneity of severe forms of this parasitosis.
Regarding retinal alterations, a previous study identified retinal pallor as the most frequent abnormality, whereas retinal haemorrhage - observed in one of our patients - was less common [36]. Brain CT scan, performed on only one of the two children, was unremarkable with no evidence of cerebral oedema. Indeed, CM is not always associated with neuroimaging alterations [37, 38], confirming the wide clinical spectrum of P. falciparum-induced cerebral damage and its diverse modes of presentation; notably, cerebral oedema typically correlates with fatal CM outcomes [39, 40]. The pulmonary consolidation in the first patient, given the negative microbiology, was likely attributable to fat embolism, a recognized cause of acute chest syndrome in children with HbS [41]. Overall, the progression to CM in these two patients likely resulted from a combination of delayed diagnosis due to the initial non-specific symptoms and high parasitaemia. Both children were successfully treated with IV artesunate, which led to a full clinical recovery without neurological sequelae. The shift from initial quinine in 2017 to direct IV artesunate in 2022 reflects the evolution of local protocols toward international gold standards. While this demonstrates improved clinical alignment, immediate access to artesunate remains a logistical challenge in some non-endemic hospitals. These cases highlight the paramount importance of early recognition: clinicians must maintain a high index of suspicion for malaria in any febrile child returning from endemic areas. Furthermore, prompt parenteral treatment and vigilant monitoring for metabolic complications are essential to ensure positive outcomes and prevent long-term disability. Indeed, our study suggests that the non-specific nature of clinical and laboratory presentations makes the early recognition of CM challenging. This supports previous observations regarding the high heterogeneity of cerebral manifestations, which do not always strictly meet WHO criteria, leading to a risk of CM underdiagnosis [30, 31, 37, 43, 44]. Therefore, identifying reliable biomarkers is pivotal for early risk stratification and effective triage of travellers returning from endemic areas. Beyond biochemical markers, current scientific efforts are focused on developing rapid prognostic tools, such as molecular tests targeting short, semi-conserved sequences like the DC8 or DC13 domains of var genes, which are closely associated with severe malaria in children and, specifically, with CM; serological tests for cerebral autoantibodies, or antibodies against PfEMP1 variants; assays measuring HRP2 levels to identify patients at higher risk of progression to CM, and tests that quantify host markers, such as Angiopoietin-2, for early detection of the extent of endothelial dysfunction within the cerebral microcirculation [44-48]. The combined use of these rapid diagnostic tools could make it possible to assess the risk of CM before the onset of neurological symptoms. However, while these specialised targets represent promising future directions, our findings demonstrate that readily available markers like PCT can already provide high-accuracy support for clinical triage. To illustrate these analytic conclusions in a real-world context, we have included two cases of paediatric CM as supportive exemplars. Rather than driving the statistical findings, these clinical narratives serve to visualize how the integration of PCT and early risk stratification can practically assist clinicians during the diagnostic dilemma of severe imported malaria. Finally, our experience underscores that CM should be carefully considered even in children with HbS trait or HbS/β-thalassaemia, despite the well-documented protection associated with these haemoglobinopathies [49-52]. The patient with HbS/β-thalassaemia had a less severe course, requiring neither prolonged antiepileptics nor ICU transfer, despite worse initial laboratory findings. However, severe malaria in this patient is noteworthy, as HbS/β-thalassaemia theoretically confers a 90% reduction in risk by limiting cytoadherence and enhancing immune tolerance [3, 53-55]. On the other hand, clinical variability in HbS heterozygotes underlines that host genetic background, pre-existing humoral immunity, and regional environmental factors significantly modulate the protective effects of HbS [53, 56]. Interestingly, studies in East India have shown that sickle cell trait carriers can remain susceptible to severe and fatal malaria at rates comparable to those of individuals with normal haemoglobin [57]. In agreement with Assohun ES et al. [58], our findings emphasize the importance of identifying genetic variants associated with the sickle cell trait, reinforcing the concept that the patient’s haemoglobin profile shapes the genetic adaptation of P. falciparum. It is also noteworthy that the patient was over 5 years of age. While literature identifies 5 years as the upper limit for maximum CM susceptibility in endemic areas [2, 3], our case suggests the importance of extending clinical attention beyond this threshold in non-immune subjects. In these patients, the absence of acquired immune memory negates age-related protection. This study has some limitations. Its retrospective, single-centre design may have introduced selection bias and limited the ability to establish causality. Despite multivariable adjustment, residual confounding cannot be excluded, and missing clinical data required a complete-case analysis, potentially affecting subgroup statistical power. Furthermore, the lack of internal validation (e.g., bootstrapping) indicates these findings remain exploratory. Nevertheless, our results reflect broader European trends, though their generalizability to different healthcare settings requires caution. Future research should focus on prospective, multicenter validation across other non-endemic contexts, standardizing data collection (e.g., PCT/CRP levels, parasite density, and WHO severity criteria) to confirm the reproducibility of our observations, particularly the predictive accuracy of PCT for severe manifestations and its impact on clinical outcomes, such as time to treatment and hospital stay.
In conclusion, our decade-long analysis reveals that imported malaria continues to represent a significant public health concern in Italy. The variable trend of severe cases, including an alarming resurgence in 2025, highlight the difficulty of statistical projection and, hence, the need for continuous surveillance and preventive measures for travellers, especially those of pre-school and school age. While both PCT and CRP levels were elevated in severe malaria, our multivariable analysis identified PCT as the more reliable independent predictor of clinical severity, whereas CRP and platelet count did not demonstrate significant prognostic value in our cohort. Combined with parasitaemia, which remains a cornerstone of assessment, PCT emerges as a robust tool for the early recognition of high-risk patients and should be prioritized in the initial triage; a high PCT level at admission should serve as a “red flag” to guide immediate clinical decisions, even when symptoms are misleadingly mild. The occurrence of two paediatric CM cases underscores that life-threatening complications persist as a tangible risk in non-endemic settings, highlighting the paramount importance of early recognition as diagnosis is often hindered by non-specific presentations. Consequently, maintaining a high index of clinical suspicion and implementing systematic risk stratification are essential. For clinicians, the prompt initiation of parenteral treatment and vigilant monitoring are crucial to ensure favorable outcomes and prevent long-term disability. Ultimately, these findings emphasize the importance of incorporating novel rapid prognostic tools into clinical practice and the need to update current guidelines with parameters that better reflect the heightened susceptibility of non-immune individuals, ensuring safer and more efficient triage in malaria-free regions.
Funding
None to declare.
Conflict of interest
The authors declare they have no conflict of interest.
REFERENCES
[1] World Health Organization (WHO). World malaria report 2025: addressing the threat of antimalarial drug resistance. Geneva: World Health Organization 2025. Available at: https://www.who.int/teams/global-malaria-programme/reports/world-malaria-report-2025. Last accessed 18 March 2026.
[2] World Health Organization. WHO guidelines for malaria, 13 August 2025. Geneva: World Health Organization 2025. Available at: https://iris.who.int/server/api/core/bitstreams/26a6af2d-060c-4449-8207-1f25e63c6cc3/content. Last accessed 18 March 2026.
[3] Williams TN, Mwangi TW, Wambua S, et al. Sickle cell trait and the risk of Plasmodium falciparum malaria and other childhood diseases. J Infect Dis. 2005; 192(1): 178-186. doi: 10.1086/430744.
[4] Garcia LS. Malaria. Clin Lab Med. 2010; 30(1): 93-129. doi: 10.1016/j.cll.2009.10.001.
[5] Trivedi S, Chakravarty A. Neurological Complications of Malaria. Curr Neurol Neurosci Rep. 2022; 22(8): 499-513. doi: 10.1007/s11910-022-01214-6.
[6] Idro R, Marsh K, John CC, et al. Cerebral malaria: mechanisms of brain injury and strategies for improved neurocognitive outcome. Pediatr Res. 2010; 68(4): 267-274. doi: 10.1203/PDR.0b013e3181eee738.
[7] Olumese PE, Gbadegesin RA, Adeyemo AA, et al. Neurological features of cerebral malaria in Nigerian children. Ann Trop Paediatr. 1999; 19(4): 321-325. doi: 10.1080/02724939992149.
[8] Molyneux ME, Taylor TE, Wirima JJ, et al. Clinical features and prognostic indicators in paediatric cerebral malaria: a study of 131 comatose Malawian children. Q J Med. 1989; 71(265): 441-459.
[9] Camponovo F, Bever CA, Galactionova K, et al. Incidence and admission rates for severe malaria and their impact on mortality in Africa. Malar J. 2017; 16(1):1. doi: 10.1186/s12936-016-1650-6.
[10] Edelu BO, Ndu IK, Igbokwe OO, et al. Severe falciparum malaria in children in Enugu, South East Nigeria. Niger J Clin Pract. 2018; 21(10): 1349-1355. doi: 10.4103/njcp.njcp_140_18.
[11] Olumese PE, Adeyemo AA, Gbadegesin RA, et al. Retinal haemorrhage in cerebral malaria. East Afr Med J. 1997; 74(5): 285-287. PMID: 9337004.
[12] Borgstein A, Zhang B, Lam C, et al. Delayed presentation to hospital care is associated with sequelae but not mortality in children with cerebral malaria in Malawi. Malar J. 2022; 21(1): 60. doi: 10.1186/s12936-022-04080-2.
[13] Associazione Microbiologi Clinici Italiani ETS (AMCLI ETS). Percorso Diagnostico - Parassitosi ematiche e del sistema reticolo endoteliale (sre) Rif. 2022-24. Available at: https://amcli.it/wp-content/uploads/2024/04/2022-24_PARASSITOSI-EMATICHE-E-DEL-SISTEMA-RETICOLO-ENDOTELIALE.pdf. Last accessed 18 March 2026.
[14] Salvadó E, Pinazo MJ, Muñoz J, et al. Presentación clínica y complicaciones de malaria importada por Plasmodium falciparum en dos grupos de población: viajeros e inmigrantes [Clinical presentation and complications of Plasmodium falciparum malaria in two populations: travelers and immigrants]. Enferm Infecc Microbiol Clin. 2008; 26(5): 282-284. Spanish. doi: 10.1157/13120415.
[15] Stano P, Arzese A, Merelli M, et al. Epidemiological and clinical features of imported malaria at the three main hospitals of the Friuli-Venezia Giulia Region, Italy. Infect Dis Health. 2018; 23(1): 17-22. doi: 10.1016/j.idh.2017.08.007.
[6] Tripathy R, Das BK, Panda AK. Procalcitonin is elevated in severe malaria and is a promising biomarker of severe malaria and multi-organ dysfunction: A cross-sectional study and meta-analysis. Int Immunopharmacol. 2023; 124(Pt A): 110923. doi: 10.1016/j.intimp.2023.110923.
[17] Wilairatana P, Mahannop P, Tussato T, et al. C-reactive protein as an early biomarker for malaria infection and monitoring of malaria severity: a meta-analysis. Sci Rep. 2021; 11(1): 22033. doi: 10.1038/s41598-021-01556-0.
[18] Chimalizeni Y, Kawaza K, Taylor T, et al. The platelet count in cerebral malaria, is it useful to the clinician? Am J Trop Med Hyg. 2010; 83(1): 48-50. doi: 10.4269/ajtmh.2010.09-0614.
[19] Patel H, Dunican C, Cunnington AJ. Predictors of outcome in childhood Plasmodium falciparum malaria. Virulence. 2020; 11(1): 199-221. doi: 10.1080/21505594.2020.1726570.
[20] Righi E, Merelli M, Arzese A, et al. Determination of PCT on admission is a useful tool for the assessment of disease severity in travelers with imported Plasmodium falciparum malaria. Acta Parasitol. 2016; 61(2): 412-418. doi: 10.1515/ap-2016-0055.
[21] Carannante N, Rossi M, Fraganza F, et al. A high PCT level correlates with disease severity in Plasmodium falciparum malaria in children. New Microbiol. 2017; 40(1): 72-74.
[22] Tielli A, Ouorou R, Pull L, et al. Might procalcitonin help predict imported falciparum malaria in children? Travel Med Infect Dis. 2024; 60: 102731. doi: 10.1016/j.tmaid.2024.102731.
[23] te Witt R, van Wolfswinkel ME, Petit PL, et al. Neopterin and procalcitonin are suitable biomarkers for exclusion of severe Plasmodium falciparum disease at the initial clinical assessment of travellers with imported malaria. Malar J. 2010; 9: 255. doi: 10.1186/1475-2875-9-255.
[24] Chiwakata CB, Manegold C, Bönicke L, et al. Procalcitonin as a parameter of disease severity and risk of mortality in patients with Plasmodium falciparum malaria. J Infect Dis. 2001; 183(7): 1161-1164. doi: 10.1086/319283.
[25] Filler S, Causer LM, Newman RD, et al.; Centers for Disease Control and Prevention (CDC). Malaria surveillance-United States, 2001. MMWR Surveill Summ. 2003; 52(5): 1-14.
[26] Kain KC, Harrington MA, Tennyson S, et al. Imported malaria: prospective analysis of problems in diagnosis and management. Clin Infect Dis. 1998; 27(1): 142-149. doi: 10.1086/514616.
[27] Bruneel F, Hocqueloux L, Alberti C, et al. The clinical spectrum of severe imported falciparum malaria in the intensive care unit: report of 188 cases in adults. Am J Respir Crit Care Med. 2003; 167(5): 684-689. doi: 10.1164/rccm.200206-631OC.
[28] Ridpath AD, Wallender E. CDC Yellow Book: Health Information for International Travel. Malaria. Edition 2026. Available at: https://www.cdc.gov/yellow-book/hcp/travel-associated-infections-diseases/malaria.html. Last accessed 18 March 2026.
[29] Schmutzhard E, Gerstenbrand F. Cerebral malaria in Tanzania. Its epidemiology, clinical symptoms and neurological long-term sequelae in the light of 66 cases. Trans R Soc Trop Med Hyg. 1984; 78(3): 351-353. doi: 10.1016/0035-9203(84)90118-4.
[30] Mishra SK, Newton CR. Diagnosis and management of the neurological complications of falciparum malaria. Nat Rev Neurol. 2009; 5(4): 189-198. doi: 10.1038/nrneurol.2009.23.
[31] Bartoloni A, Zammarchi L. Clinical aspects of uncomplicated and severe malaria. Mediterr J Hematol Infect Dis. 2012; 4(1): e2012026. doi: 10.4084/MJHID.2012.026.
[32] Chiabi A, Obadeyi B, Nguefac S, et al. Seizures in Severe Malaria: Is there Direct Brain Involvement? The Open Area Studies Journal. 2011; 4(1): 1-6.
[33] Kawo NG, Msengi AE, Swai AB, et al. Specificity of hypoglycaemia for cerebral malaria in children. Lancet. 1990; 336(8713): 454-457. doi: 10.1016/0140-6736(90)92009-7.
[34] Madrid L, Lanaspa M, Maculuve SA, Bassat Q. Malaria-associated hypoglycaemia in children. Expert Rev Anti Infect Ther. 2015; 13(2): 267-277. doi: 10.1586/14787210.2015.995632.
[35] Chastang KM, Imam R, Sherman MG, et al. Temporal Trends of Blood Glucose in Children with Cerebral Malaria. Am J Trop Med Hyg. 2023; 108(6): 1151-1156. doi: 10.4269/ajtmh.23-0022.
[36] Jegede TO, Oseni SB, Okeniyi JAO, et al. Pattern of Clinical and Laboratory Presentation of Cerebral Malaria among Children in Nigeria. J Glob Infect Dis. 2024; 16(1): 5-12. doi: 10.4103/jgid.jgid_100_23.
[37] Newton CR, Peshu N, Kendall B, et al. Brain swelling and ischaemia in Kenyans with cerebral malaria. Arch Dis Child. 1994; 70(4): 281-287. doi: 10.1136/adc.70.4.281.
[38] Dubey A, Dubey S, Dhawale RG. Study of Computed Tomography in Patients of Cerebral Malaria. J Neurol Exp Neural Sci. 2017; JNNS-132.
[39] Seydel KB, Kampondeni SD, Valim C, et al. Brain swelling and death in children with cerebral malaria. N Engl J Med. 2015;372(12):1126-37. doi: 10.1056/NEJMoa1400116.
[40] Taylor TE, Molyneux ME. The pathogenesis of pediatric cerebral malaria: eye exams, autopsies, and neuroimaging. Ann N Y Acad Sci. 2015; 1342(1): 44-52. doi: 10.1111/nyas.12690.
[41] Vichinsky EP, Neumayr LD, Earles AN, et al. Causes and outcomes of the acute chest syndrome in sickle cell disease. National Acute Chest Syndrome Study Group. N Engl J Med. 2000; 342(25): 1855-1865. doi: 10.1056/NEJM200006223422502.
[42] Schumacher RF, Spinelli E. Malaria in children. Mediterr J Hematol Infect Dis. 2012;4(1): e2012073. doi: 10.4084/MJHID.2012.073.
[43] Guenther G, Muller D, Moyo D, et al. Pediatric Cerebral Malaria. Curr Trop Med Rep. 2021; 8(2): 69-80. doi: 10.1007/s40475-021-00227-4.
[44Lavstsen T, Turner L, Saguti F, et al. Plasmodium falciparum erythrocyte membrane protein 1 domain cassettes 8 and 13 are associated with severe malaria in children. Proc Natl Acad Sci U S A. 2012; 109(26): E1791-800. doi: 10.1073/pnas.1120455109.
[45] Bansal D, Herbert F, Deshpande P, et al. Auto-antibodies targeting brain antigens in Plasmodium falciparum infected patients as biomarkers of Cerebral Malaria. Malar J. 2010; 9(Suppl 2): P4. doi: 10.1186/1475-2875-9-S2-P4.
[46 Dalgaard N, Olsen RW, Adams Y, et al. A monoclonal antibody selectively recognizing PfEMP1 proteins associated with cerebral malaria. Sci Rep. 2025; 15(1): 34732. doi: 10.1038/s41598-025-18465-1.
[47] Fox LL, Taylor TE, Pensulo P, et al. Histidine-rich protein 2 plasma levels predict progression to cerebral malaria in Malawian children with Plasmodium falciparum infection. J Infect Dis. 2013; 208(3): 500-503. doi: 10.1093/infdis/jit176.
[48] Conroy AL, Glover SJ, Hawkes M, et al. Angiopoietin-2 levels are associated with retinopathy and predict mortality in Malawian children with cerebral malaria: a retrospective case-control study. Crit Care Med. 2012; 40(3): 952-959. doi: 10.1097/CCM.0b013e3182373157.
[49] Abah MA, Archibong EU, Oladosu MA, et al. The protective role of sickle cell trait against Plasmodium falciparum malaria. J Hum Virol Retrovirol. 2025; 12(1): 23-31. doi: 10.15406/jhvrv.2025.12.00283.
[50] Ayi K, Turrini F, Piga A, et al. Enhanced phagocytosis of ring-parasitized mutant erythrocytes: a common mechanism that may explain protection against falciparum malaria in sickle trait and beta-thalassemia trait. Blood. 2004; 104(10): 3364-3371. doi: 10.1182/blood-2003-11-3820.
[51] Huang R, Li X, Lu Z, et al. Thalassemia carriers exhibit reduced expression of the receptor for the malarial parasite Plasmodium vivax on erythrocytes. Blood Adv. 2025; 9(7): 1738-1741. doi: 10.1182/bloodadvances.2024014792.
[52] Olumese PE, Adeyemo AA, Ademowo OG, et al. The clinical manifestations of cerebral malaria among Nigerian children with the sickle cell trait. Ann Trop Paediatr. 1997; 17(2): 141-145. doi: 10.1080/02724936.1997.11747877.
[53] Cholera R, Brittain NJ, Gillrie MR, et al. Impaired cytoadherence of Plasmodium falciparum-infected erythrocytes containing sickle hemoglobin. Proc Natl Acad Sci U S A. 2008; 105(3): 991-996. doi: 10.1073/pnas.0711401105.
[54] Luzzi GA, Merry AH, Newbold CI, et al. Surface antigen expression on Plasmodium falciparum-infected erythrocytes is modified in alpha- and beta-thalassemia. J Exp Med. 1991;173(4): 785-791. doi: 10.1084/jem.173.4.785.
[55] Ferreira A, Marguti I, Bechmann I, et al. Sickle hemoglobin confers tolerance to Plasmodium infection. Cell. 2011; 145(3): 398-409. doi: 10.1016/j.cell.2011.03.049.
[56] Agarwal A, Guindo A, Cissoko Y, et al. Hemoglobin C associated with protection from severe malaria in the Dogon of Mali, a West African population with a low prevalence of hemoglobin S. Blood. 2000; 96(7): 2358-2363. PMID: 11001883.
[57] Pati SS, Panigrahi J, Mishra SK, Mohanty S, Mohapatra DN, Das BS. Severe complications and death in cases of Plasmodium falciparum malaria with sickle-cell trait. Ann Trop Med Parasitol. 2005; 99(3): 317-320. doi: 10.1179/136485905X28036.
[58] Assohoun ES, Kouassi BM, Ako AB, et al. Multivariate Statistical analysisof the genetic diversity of Plasmodium falciparum isolates from individuals carrying the major or minor sickle cell trait (HBAA, HBAS, and HBSS) in Abidjan (Cote d’Ivoire): application of principal component analysis, Jost’s D Index and PERMANOVA. Open Journal of Applied Sciences. 2025; 15: 1716-1731.