Le Infezioni in Medicina, n. 3, 249-260, 2025
doi: 10.53854/liim-3303-1
REVIEWS
The burden of infections caused by Metallo-Beta-Lactamase-Producing Enterobacterales in Italy: epidemiology, outcomes, and management
Giusy Tiseo1, Stefania Stefani2, Francesca Romana Fasano3, Marco Falcone1
1Infectious Diseases Unit, Department of Clinical and Experimental Medicine, Azienda Ospedaliera Universitaria Pisana, University of Pisa, Pisa, Italy;
2Department of Biomedical and Biotechnological Sciences, University of Catania, Catania, Italy;
3Medical Affairs, Pfizer Italia, Rome, Italy.
Article received 25 May 2025 and accepted 21 August 2025
Corresponding author
Marco Falcone
E-mail: marco.falcone@unipi.it
SummaRY
Metallo-β-lactamase (MBL)-producing Enterobacterales represent a growing public health threat due to their intrinsic resistance to several antibiotics. In Italy, the burden of infections caused by these organisms has been steadily increasing. In recent years, MBL-producing Klebsiella pneumoniae, particularly those carrying New Delhi metallo-β-lactamase (NDM) enzyme, have emerged across multiple Italian regions, frequently associated with high-risk clones such as ST147. These infections are associated with high morbidity, mortality, and healthcare costs. While advances in diagnostic techniques have improved the detection of MBLs, underreporting and heterogeneous practices are common. Therapeutic options remain limited.
The rising incidence and clinical complexity of MBL-producing Enterobacterales in Italy underscore the urgent need for coordinated actions to improve surveillance, diagnostics, infection control, and optimize antimicrobial stewardship. The development of novel therapeutic agents and the implementation of strategies for managing MBLs are crucial to reduce their clinical and public health impact. This review aims to provide a comprehensive overview of the current epidemiology, clinical outcomes, and management challenges of infections caused by MBL-producing Enterobacterales in Italy.
Keywords: Antimicrobial resistance, Epidemiology, Klebsiella pneumoniae NDM, Metallo-β-lactamase-producing Enterobacterales.
INTRODUCTION
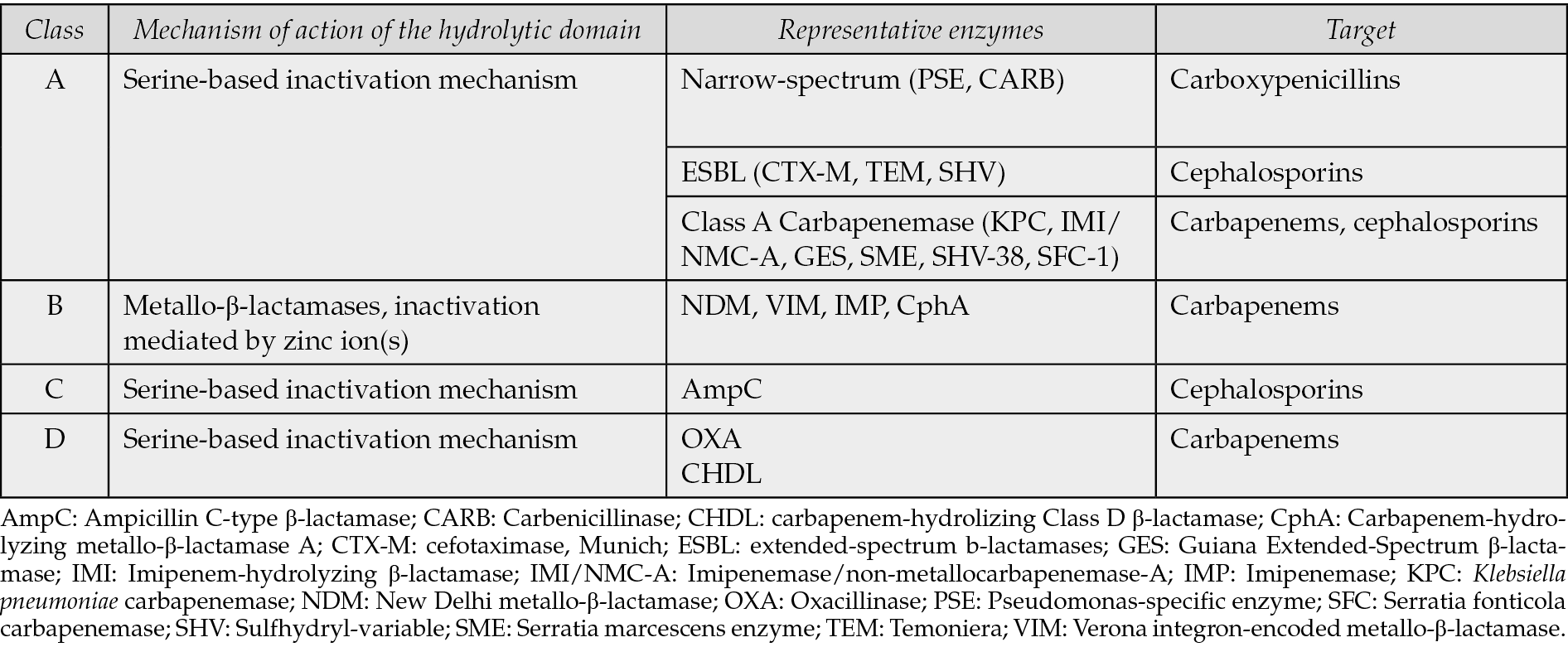
Carbapenem-resistant Enterobacterales (CRE), including Klebsiella pneumoniae (K. pneumoniae) and Escherichia coli (E. coli), represent a great challenge worldwide [1]. Their resistance is largely mediated by the production of carbapenemases, as reported in Table 1 [2]. However, this is not a unique resistance mechanism. Multiple mechanisms including efflux pump overexpression and porin loss have been implicated in carbapenem resistance among Enterobacterales. These co-existing resistance determinants, often harbored within the same strain, significantly complicate phenotype of resistance.
Table 1 - Molecular classification of the ß-lactamases enzymes (Ambler classification).
MBL-producing CRE pose a global health threat due to limited therapeutic options and high attributable mortality, especially in elderly and immunocompromised patients [3-7]. The economic burden of these infections is also considerable, since they are associated with prolonged hospital stays and increased healthcare costs [8]. The global spread of these resistant pathogens, mainly driven by dominant clonal complexes, is largely facilitated by horizontal gene transfer which promotes the persistence and diversification of resistance genes across different bacterial hosts [9]. With regards to species, both carbapenem-resistant K. pneumoniae and E. coli represent a threat for human health. However, recent studies have highlighted the growing clinical concern posed by MBL-producing E. coli, particularly in the context of urinary tract infections (UTI) [10-12]. In fact, uropathogenic E. coli are characterized by substantial genetic heterogeneity, high prevalence of carbapenemase-encoding genes (including blaNDM and blaOXA variants), and enhanced biofilm-forming capacity [10-11]. This pathogen is increasingly detected in immunocompromised patients, such as kidney transplant recipients, and can be related to poor clinical outcome [10].
In recent years, the epidemiological landscape is changing with a global increase in the MBL detection among CRE. Until 2018, K. pneumoniae carbapenemase (KPC) was the predominant carbapenemase in the United States and Europe, including Italy [13-15]. However, the ATLAS study (2018-2019) showed regional variation in MBL prevalence, with rates of 59.4% in Asia–Pacific and 49% in Africa/Middle East [16]. In the US, KPC prevalence declined from 73.8% in 2019 to 57.1% in 2021, whereas MBLs increased from 3.8% to 20.4% [17]. Moreover, 7.8% of meropenem-nonsusceptible Enterobacterales co-produced two carbapenemases, most commonly NDM and OXA-48-like carbapenemases [16]. Although outbreaks of MBL-producing Enterobacterales have been reported in Italy, national surveillance data remain limited, highlighting the need for updated epidemiological insight [5, 14, 18-20].
This review aims to provide an updated summary of the epidemiology, infection outcomes, and clinical impact of MBL-producing Enterobacterales in Italy.
METHODS
A comprehensive literature search was conducted using PubMed to identify relevant studies on infections caused by MBL-producing Enterobacterales in Italy published in the last 15 years. The studies were retrieved using the logical combinations of the search terms “Infections”, “Metallo-beta-lactamase”, “Klebsiella pneumoniae”, “Enterobacterales”, “Enterobacteriaceae”, “carbapenem-resistant Enterobacterales”, “CRE” and “Italy”. Inclusion criteria focused on epidemiology, treatment outcomes, management and surveillance of MBL-producing Enterobacterales in Italy. Data from these studies were summarized in this narrative review to provide an overview of the burden, transmission, and clinical management of these infections.
EPIDEMIOLOGY
The recently published risk assessment by the European Centre for Disease Prevention and Control (ECDC) reported a 10.2% increase in the incidence of bloodstream infections (BSI) caused by carbapenem-resistant K. pneumoniae in Italy between 2019 and 2023 [21]. The most recent Italian National Surveillance report describes 3,867 cases of BSI caused by CRE in 2023 compared to 2,183 in 2016, with the highest incidence observed in Central Italy, followed by the South and Islands, and the North [6]. These infections are predominantly linked to urinary tract and central/peripheral venous catheters [6].
In 74.9% of cases, KPC was identified as the enzyme responsible for carbapenem resistance, whereas MBL enzymes were detected in 13.8% of cases, marking an increase from 8.4% reported in 2022. NDM and VIM represented 89% and 9% of the total MBL respectively [6]. NDM-producing K. pneumoniae was mostly identified in Lombardy, Tuscany, Piedmont, Sicily, and Apulia, where multiple hospitals have reported outbreaks [5, 6, 22, 23].
The first outbreak of NDM-1-producing sequence type (ST) 147 K. pneumoniae emerged in the North-Western area of the Tuscany region in late 2018 and was associated with an increase in BSI during 2019–2020 [19, 22, 23]. Subsequently, other outbreaks have been documented from 2020 to 2022 in Apulia (22.6% of isolates with NDM-producing K. pneumoniae), and more recently in Pavia area, where an NDM-producing K. pneumoniae clone ST6668 rapidly spread across hospitals [19, 24].
The NDM-producing K. pneumoniae ST147 linked to the Tuscany outbreak has been extensively characterized [23, 25]. Susceptibility to aztreonam-avibactam was reported in 99.7% of cases, whereas susceptibility to aminoglycosides, fosfomycin and tigecycline was detected in 30%, 67% and 70.9% of isolates, respectively [5]. Fully susceptibility to cefiderocol according to 2023 EUCAST breakpoints was detected in 33.2% of cases, whereas the 69.2% of isolates had an alone of inhibition in the area of technical uncertainty [5].
Co-existence of different resistance genes encoding carbapenemases within the same strain has been reported [26-30]. The simultaneous presence of multiple carbapenemases in invasive isolates is increasing, suggesting an evolutionary advantage [26-30]. Co-infections involving NDM and OXA-48 are becoming more frequent, particularly in K. pneumoniae strains [18, 29, 31]. In Italy, 3.4% cases of BSIs with simultaneous carbapenemase were reported in 2023 with respect to 2.6% in 2022 [8]. Recently, NDM-1/OXA-48 coproducing- K. pneumoniae isolates from BSI have been reported in Calabria region [31]. In all the strains, beta-lactamases resistance genes, blaOXA-48, blaNDM-1, blaCTX-M-15, and blaSHV, were found. Most of the NDM-1/OXA-48 producing K. pneumoniae strains belonged to the high-risk clone ST147 [31].
Another study reported the first documented case in Italy of a K. pneumoniae strain carrying three different carbapenemases, NDM-1/5, and OXA-48, on separate plasmids, isolated in Milan in 2019 [18]. All isolates were resistant to almost all antibiotics available at that time, except for colistin and tigecycline [18]. Co-expression of multiple carbapenemases was found also in a study from Apulia, with 11 isolates out of 459 displaying NDM + KPC, and one isolate KPC + VIM [23] (Figure 1).
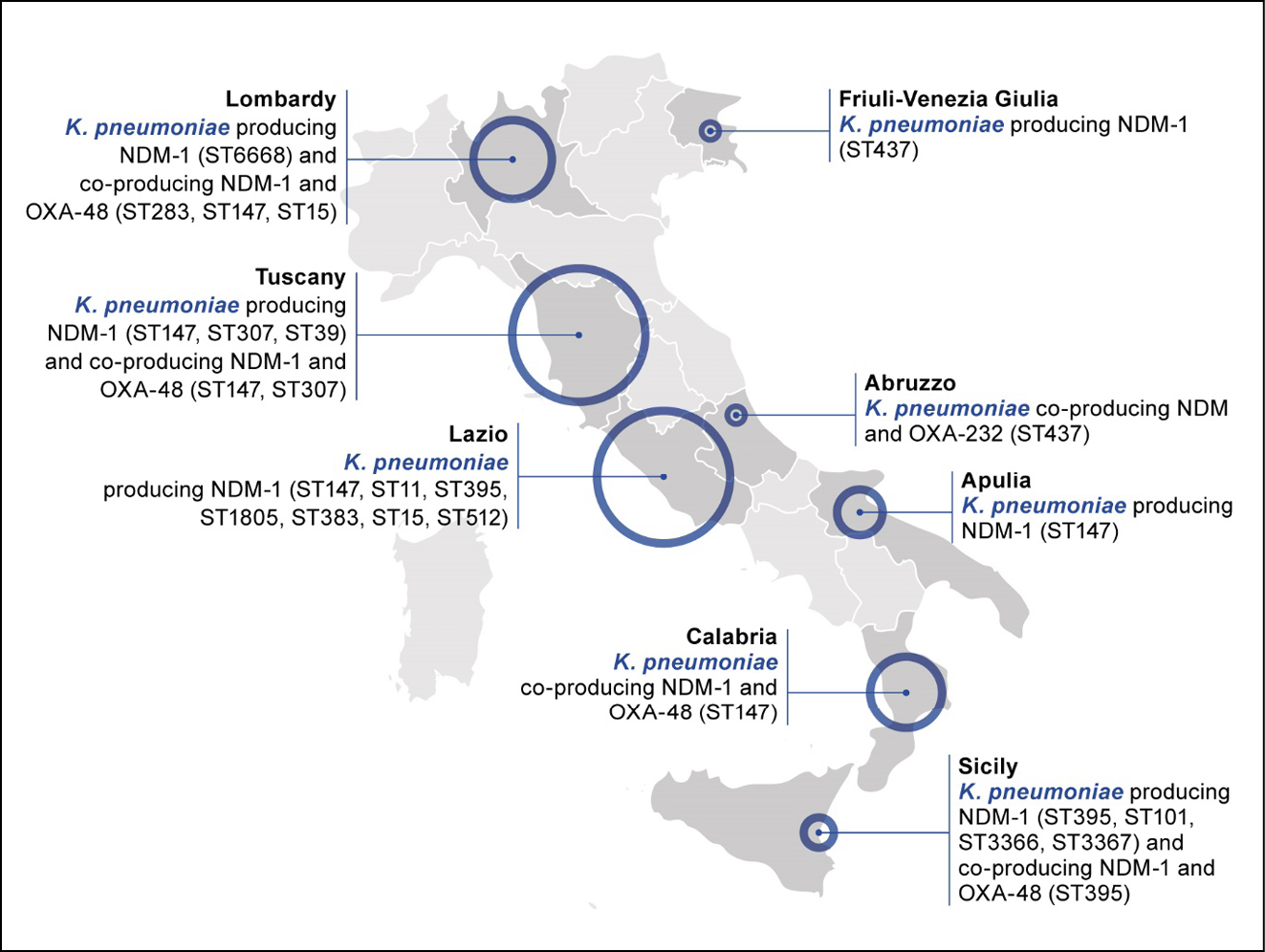
Figure 1 - Geographic distribution of selected outbreaks of NDM-1 producing K. pneumoniae across Italy (2018-2023).* The figure includes only isolates for which clone type (ST) was specified according to [5, 18, 19, 23, 27, 28, 31, 41, 61]. *ST147 NDM1-producing Klebsiella pneumoniae is endemic in the Tuscany region, whereas other clones have been sporadically detected.
Resistance genes such as blaNDM, often carried on mobile genetic elements like IncX3 plasmids, can spread easily between bacteria. The presence of multiple plasmids and the rapid transfer of resistance genes increase the risk of spreading resistance to other K. pneumoniae strains or different Enterobacterales. This amplifies the potential for outbreaks in intensive care units (ICUs) and hospital wards, making infections more difficult to treat, and underscoring the need for infection control measures to prevent transmission [32].
Of importance, MBL are increasingly detected not only among K. pneumoniae isolates [7, 33-35]. A recent study reported a nosocomial outbreak of VIM-producing Enterobacterales that occurred in an Italian medical unit from November 2021 to December 2023. The spread involved several different species of Enterobacterales, including K. oxytoca, Enterobacter cloacae, Citrobacter freundii [35]. These reports highlight the evolving epidemiological landscape beyond K. pneumoniae.
Although most infections caused by CRE occur in the hospital settings, community-acquired infections are alarmingly increasing becoming a threat especially in frail patients. For instance, residents in long-term facilities are at higher risk for the potential broad antibiotic use [36-39]. Long-term care facilities were identified as hotspots for the spread of CRE, emphasizing the need for implementing infection control measures, including efficient disinfection protocols and systematic rectal screening in hospitals as well as in nursing homes to reduce patients’ transmission [36-39].
According to national surveillance data, 18.7% of BSI caused by CRE in Italy in 2023 had their onset at home, and 6.9% occurred in residential care facilities, confirming that a significant proportion of CRE-BSI originate outside of hospitals [6]. Some studies showed that NDM-producing CRE spread in the community and may be responsible for incident cases of infections in patients admitted to Emergency Department [40].
ENVIRONMENTAL SOURCES
Environmental reservoirs play a critical role in the transmission of MBL-producing Enterobacterales, particularly in the context of prolonged or recurring outbreaks. Environmental surfaces can harbor biofilm-associated populations of CRE. These niches support bacterial survival and promote horizontal gene transfer, making them ideal settings for sustained colonization by multidrug-resistant strains. Environmental contamination can lead to indirect patient-to-patient transmission through splashes, aerosols, or contaminated hands and equipment, even in the absence of direct contact. Environmental niches, such as sink drains or water systems, can sustain long-term colonization by CRE, facilitating indirect patient-to-patient transmission and contributing to the transition from epidemic to endemic spread.
Environmental persistence can favor hospital dissemination of MBL-CRE, in particular of VIM-producing isolates. In fact, the study by Oliveri et al highlighted the role of environmental persistence in the spread of MBL-CRE in hospital settings [35]. In this study, the implementation of increasingly aggressive infection control practices was apparently able to temporarily mitigate the spread of VIM-CRE but not to eradicate the phenomenon, which was likely supported by an environmental reservoir of VIM-positive strains [35]. Environmental VIM-positive isolates were ubiquitous in sinks in the ward but with a prevalent distribution in the rooms most distant from the waste disposal, potentially indicating an improper use of sinks for the disposal of body fluids from colonized patients [35]. Therefore, routine environmental screening and targeted interventions, including enhanced cleaning protocols, water system decontamination and implementation of infection control measures should be considered integral components of infection prevention and control strategies.
COLONIZATION AND RISK OF PROGRESSION TO INFECTION
Intestinal colonization with carbapenem-resistant K. pneumoniae represents a critical precursor to invasive infections in hospitalized patients [40, 41]. Among patients in high-risk units (i.e., Intensive Care and Neonatal Intensive Care Units, Haematology Unit, Emergency Room, and Neurological Clinic), 4.9% developed BSI caused by the same intestinal colonizing strains [41]. The concordance between rectal and blood samples strains was confirmed by whole genome sequencing through analysis of sequence type, resistance and virulence genes, and plasmid profile [41]. This detailed analysis allowed the recognition of the ST101 and ST395 as emerging invasive clones over the conventional ST258/ST512. Moreover, this study reinforced asymptomatic gastro-intestinal colonization as a reservoir for potential subsequent invasive infections, especially in ICU and immunocompromised patients [40, 41].
The risk of progression from intestinal colonization to invasive infection is a key concern in patients with colonization by MBL-producing Enterobacterales. A recent national systematic review estimated an overall progression rate from colonization to infection among CRE carriers of 11% [42]. Notably, the risk varied substantially across bacterial species and healthcare settings, with higher rates reported for K. pneumoniae and among patients in intensive care units and onco-hematology wards. Moreover, intestinal colonization by CRE can be associated with different risk of BSI depending on the carbapenemase type [40]. The CHIMERA study, which included 677 rectal carriers of carbapenemase-resistant K. pneumoniae of whom 56.4% were NDM, 36.5% KPC, 5.8% VIM, and 1.8% OXA-48, found that the risk of BSI differed by carbapenemase type. Specifically, patients with rectal colonization by NDM‒producing K. pneumoniae had higher risk of BSI compared to KPC rectal carriers (59/382, 15.4% versus 20/247, 8.1%, respectively, p=0.004) [40]. The incidence rates of BSI per 100 patients per month was significantly higher in the NDM group (22.33, 95% CI 17.26-28.88) than in the KPC group (9.56, 95% CI 6.17-14.82), suggesting that the type of carbapenemase may influence the risk of subsequent BSI [40]. This higher incidence of BSI in the NDM group seems to be mainly related to an increased virulence of the ST147 NDM clone [40].
The knowledge of colonization status may be useful to identify carriers and, consequently, implement infection control measures and guide the choice of an appropriate empirical therapy when septic shock occurs [12]. Although universal colonization screening is not routinely implemented, routine rectal screening for CRE may be useful in high-risk hospital wards, e.g. onco-hematology and ICUs, in subjects with immunosuppression (e.g. transplant and oncological patients), in patients with septic shock, and in epidemiological setting endemic for different carbapenemases (KPC vs NDM vs OXA-48) [40]. Further studies are needed to better delineate the contexts in which molecular rectal screening should be implemented.
OUTCOMES
BSI by MBL-producing CRE are associated with poor patients’ outcomes [3-5, 21, 38-40]. The highest mortality rates have been reported in elderly patients hospitalized in internal medicine units and in ICU [43-45]. A recent study including 30 patients with NDM-Kp BSI hospitalized in internal medicine reported a 30-day mortality rate as high as 46.7% [43]. Of importance, urinary tract infections by NDM-producing CRE are associated with treatment failure in elderly patients, underscoring the impact of antimicrobial resistance in this high-risk population [44]. In ICU setting, patients with infections due to NDM-producing Enterobacterales had both a mortality rate and a treatment failure rate of 37.5% in the ICU [45].
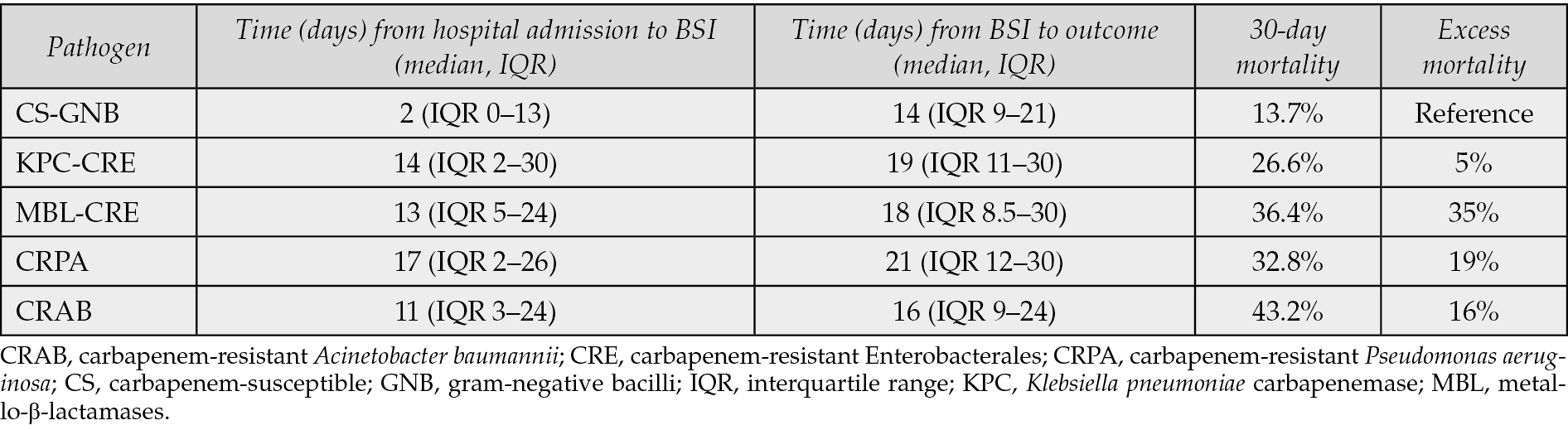
In the ALARICO study, which included more than 1000 cases of BSI due to carbapenem-resistant Gram-negative bacilli in Italy, the highest attributable mortality was observed in patients with MBL-producing Enterobacterales (35%), followed by carbapenem-resistant A. baumannii (16%), carbapenem-resistant P. aeruginosa (19%), and KPC-producing K. pneumoniae (5%) [3] (Table 2). These data highlight the poor prognosis associated with MBL-related infections. In the ALARICO study nearly two-thirds of patients with NDM received colistin-containing regimens, that may have contributed to the high mortality rates in this group [3]. On the contrary, most of KPC received ceftazidime/avibactam, highlighting that the choice of antibiotic may contribute to the clinical outcome of patients with CRE BSI. Moreover, these findings reflect the broader challenge in managing MBL-BSI in the absence of effective targeted therapies during the study period. Delays in appropriate treatment and limited access to active agents likely played a key role in the high mortality rates observed. These results reinforce the clinical need for early identification of MBL-producing strains and access to novel therapeutic agents, which can offer promising activity against these difficult-to-treat pathogens. Recent evidence supports this observation. A multicenter retrospective cohort study conducted in seven hospitals in Italy and Israel investigated the association between carbapenemase type (NDM vs KPC vs OXA-48) and 30-day mortality in patients with BSIs caused by CRE [46]. The authors found no difference in mortality rates between carbapenemase groups, suggesting that differences in clinical outcomes may be more strongly influenced by host factors and treatment appropriateness than by the specific carbapenemase type itself [46].
One of the major determinants of outcome in patients with BSI by CRE is represented by the timing of appropriate antibiotic therapy, that should be started as early as possible, ideally within the first 24 hours following blood culture collection [47]. Thus, inadequate molecular diagnostics, relying solely on phenotypic resistance information, further complicates treatment and contributes to delayed therapy [48].
Table 2 - Summary of time from hospital admission to BSI, time from BSI to outcome and 30-day mortality of infections caused by different carbapenem-resistant Gram-negative bacilli from the ALARICO Study [3].
DIAGNOSTIC TESTS IN ITALY
Improved laboratory capabilities for detecting carbapenemase types have advanced understanding of CRE epidemiology and colonization, enabling targeted interventions. However, underreporting and inconsistencies in surveillance protocols across Italy may influence the actual burden of MBL-producing Enterobacterales [6].
Detection of carbapenemases is required for patient management, rapid implementation of infection prevention and control protocols, and epidemiologic purposes. Therefore, microbiology laboratories must be able to detect and report carbapenemases among Gram-negative organisms from both cultured isolates and directly from clinical specimens for treatment and surveillance purposes.
Detection methods for β-lactamase can be classified into three groups: those based on phenotypic detection, those based on the hydrolysis by β-lactamase, and β-lactamase gene detection. For a detailed description of these methods refer to review papers [2, 49].
Rapid immunochromatographic methods, such as lateral flow assays, designed to detect specific carbapenemase enzyme family, have been increasingly used and in some cases they are applied to accurately detect these enzymes from positive blood cultures and direct rectal swabs [50-52]. CLSI guidelines emphasize the importance of using phenotypic assays to identify and differentiate specific carbapenemase types and suggest a stepwise approach for carbapenemases detection, prioritizing phenotypic methods for initial screening and then using genotypic methods for confirmation and identification of specific carbapenemase types.
The modified carbapenem inactivation method (mCIM) and EDTA-modified carbapenem inactivation method (eCIM) are indicated to distinguish serine-beta-lactamases from MBLs [53]. EUCAST underlines the importance of screening for resistance mechanisms of epidemiological and infection control importance [54]. Molecular methods and lateral flow assays for the rapid identification and characterization of carbapenemase types are recommended. These methods offer faster results compared to traditional culture-based methods. Sullivan E and colleagues compared the NG-Test Carba-5 lateral flow assay against a PCR-based molecular method (Cepheid Xpert Carba-R) for detecting carbapenemase genes (blaKPC, blaNDM, blaVIM, blaIMP, blaOXA-48) [55]. The results showed 98.2% overall agreement and a significantly faster turnaround time [55].
Moreover, matrix-assisted laser desorption ionization-time of flight mass spectroscopy (MALDI-TOF MS) is emerging as a promising tool for direct CRE detection from blood samples and epidemiological surveillance [48].
In many Italian hospitals, molecular testing for the detection of carbapenemase genes, primarily targeting the five major ones (blaKPC, blaNDM, blaOXA-48-like, blaIMP, blaVIM) is a key diagnostic tool used both at hospital admission and during hospitalization [40, 56]. Automated commercial molecular assays have the advantage of simplified workflow and procedures that can be performed with minimal molecular expertise and many of them demonstrated good performance with excellent sensitivity and specificity [57].
EMERGING LANDSCAPE OF THERAPEUTIC STRATEGIES AGAINST MBL-CRE
Effective management of CRE infections requires coordinated regional efforts to improve surveillance and implement robust infection control measures [6]. At the same time, the evolution of treatment options plays a critical role in improving patient outcomes [58, 59].
Very limited therapeutic options are currently available for the treatment of infections caused by MBL-CRE. They include old (colistin, fosfomycin or tigecycline) and new (aztreonam/avibactam and cefiderocol) antibiotic regimens.
Historically, colistin was the cornerstone of treatment, but its use has decreased due to toxicity and suboptimal efficacy [3]. Cefiderocol is a potential option, but concerns about reduced susceptibility, in particular against NDM-1 producing Enterobacterales, may limit its use, especially as empirical treatment [5, 60-63].
A recent epidemiological study showed that, using the EUCAST breakpoints, the prevalence of cefiderocol-non susceptible strains is higher among CRE compared to non-fermenting Gram negative bacilli, such as P. aeruginosa [64]. More specifically, cefiderocol non-susceptibility was exceedingly high in NDM-producing Enterobacterales (38.8%) [64]. In Italy, an outbreak reported in Florence involved 21 strains of NDM-1-producing Enterobacterales resistant to cefiderocol out of a total of 52 recorded between August 2021 and July 2022 [60]. This occurred regardless of prior exposure to the drug, thus demonstrating that cefiderocol-resistant strains do not necessarily exhibit fitness defects and can spread even in the absence of direct selective pressure [60]. The largest observational study on MBL conducted in Pisa reported that up to 66.8% of MBL-producing Enterobacterales were resistant to cefiderocol [5]. A recent publication from Udine described the emergence of cefiderocol resistance in an NDM-1-producing K. pneumoniae strain following treatment, along with its subsequent intra-hospital spread [61]. In Genoa, cefiderocol resistance was also reported in clinical isolates from pediatric patients with no prior exposure to the drug: 16 out of 30 tested Enterobacterales strains (mostly MBL producers) were found to be resistant [65].
Aztreonam-avibactam (ATM-AVI) is an emerging option for treating MBL infections recently approved by EMA [66-70]. This treatment combines the stability to MBLs of aztreonam with the inhibition ability of avibactam against wide range of beta-lactamases, including extended-spectrum beta-lactamases (ESBLs) that are often co-expressed by MBL-producing bacteria [10, 71]. The molecule showed an in vitro broad activity against multi-resistant Enterobacterales, including MBL-producing strains, with a lower prevalence of resistant strains compared to other combined compounds and cefiderocol [72-74]. A multicenter in vitro study conducted in 21 European countries, which included meropenem-resistant Enterobacterales strains collected in 2020, showed susceptibility rate to cefiderocol of 75% and to ATM-AVI of 99% [75]. Notably, among cefiderocol-resistant strains (one third of which originated from Italy and frequently harbored multiple resistance mechanisms) 94.6% remain susceptible to ATM-AVI, underscoring both the possible differences in susceptibility profiles between the two agents, and the clinical value of retaining both as therapeutic options [75].
Another agent undergoing evaluation is cefepime-taniborbactam, which combines a
cephalosporin with a β-lactamase inhibitor, that demonstrates potent activity against a broad range of β-lactamases, including class A (e.g., KPC), class C, class D, and several class B β-lactamases such as NDM [76]. However, its activity does not extend to all MBLs, as it shows limited or no activity against IMP-type carbapenemases, highlighting the importance of molecular characterization when selecting targeted therapy [59]. Other two investigational β-lactam/β-lactamase inhibitor combinations, cefepime/zidebactam and cefepime/nacubactam, have shown promising in vitro activity against MBL-producing Enterobacterales. Zidebactam acts both as a β-lactamase inhibitor and as a β-lactam enhancer by binding to PBP2, which enhances the activity of cefepime even in the presence of MBL. Similarly, nacubactam also inhibits serine β-lactamases (including ESBLs and AmpC) and enhances cefepime activity by PBP2 binding [59].
Of particular concern is the emerging co-production of VIM and mobilized colistin resistance (mcr) genes in Enterobacterales, which significantly limits therapeutic options [77]. The simultaneous presence of carbapenemase- and colistin-resistance mechanisms confers resistance to two major last-resort antibiotic classes, leaving few or no effective treatments available.
Overall, data from clinical studies on MBL-producing Enterobacterales are still limited and studies to investigate further therapeutic options are warranted [78, 79].
CONCLUSIONS
The rising prevalence of MBL-producing Enterobacterales in Italy, once confined to localized outbreaks, now demands broader clinical awareness. Rectal colonization remains the main risk factor, supporting the implementation of rectal screening in high-risk wards and, when possible, its extension to other healthcare settings. Hospital-level surveillance, with timely data sharing, is essential to guide infection management.
The rising prevalence and complexity of MBL-producing Enterobacterales infections in Italy highlight the urgent need for integrated infection prevention strategies. These should combine routine molecular surveillance, including whole-genome sequencing, with environmental diagnostics to detect hidden reservoirs, and targeted antimicrobial stewardship to guarantee the optimal therapeutic options in infected patients. Coordinated efforts at both the hospital and national level are essential to prevent the further spread of these difficult-to-treat organisms and to mitigate their clinical and public health impact.
Author contribution
All authors conceived the study, analyzed the literature, wrote, edited, and critically revised the manuscript. All authors approved the current version for submission
Conflicts of interest
GT received speaker honoraria by Shionogi, Gilead, Menarini, Pfizer and honoraria for participation on a scientific board from MSD and Advanz Pharma. MF received unconditional grants from Gilead and speaker honoraria from Shionogi, Pfizer, Menarini, MSD, Gilead, GSK, MundiPharma, and Thermo Fisher.
SS received speaker honoraria from Menarini, Pfizer, BD, Biomerieux; she received study grant from Angelini, Shionogi, Infectofos.
FRF is a Pfizer employee.
Funding
G.T., S.S., M.F. were paid consultants to Pfizer in connection with the development of this manuscript. The medical writing support was provided by Ahana Maitra at Health Publishing and Services and was funded by Pfizer. Editorial support was provided by Barbara Bartolini at Health Publishing and Services and was funded by Pfizer.
REFERENCES
- Nordmann P, Poirel, L. Epidemiology and diagnostics of carbapenem resistance in Gram-negative bacteria. Clin Infect Dis. 2019; 69: S521-S528.
- Simner PJ, Pitout JDD, Dingle TC. Laboratory detection of carbapenemases among Gram-negative organisms. Clin Microbiol Rev. 2024; 37(4): e0005422.
- Falcone M, Tiseo, G, Carbonara, S, et al. Mortality attributable to bloodstream infections caused by different carbapenem-resistant gram-negative bacilli: results from a nationwide study in Italy (ALARICO Network). Clin Infect Dis. 2023; 76(12): 2059-2069.
- Tiseo G, Galfo, V, Carbonara, S, et al. Bacteremic nosocomial pneumonia caused by Gram-negative bacilli: results from the nationwide ALARICO study in Italy. Infection. 2025; 53(3): 1041-1050.
- Falcone M, Giordano, C, Leonildi, A, et al. Clinical features and outcomes of infections caused by metallo-beta-lactamase-producing Enterobacterales: a 3-year prospective study from an endemic area. Clin Infect Dis. 2024; 78(5): 1111-1119.
- Iacchini S, Fadda, G, Monaco, M, et al. CRE: sorveglianza nazionale delle batteriemie da enterobatteri resistenti ai carbapenemi. Dati 2023 2024. https://www.iss.it/documents/20126/9840005/RIS+4_2024.pdf/eb0ac8a0-3b4f-a3eb-d21a-fcbc87cc98ff?t=1734614842867 (Accessed 20 May 2025).
- Falcone M, Mezzatesta, ML, Perilli, M, et al. Infections with VIM-1 metallo-beta-lactamase-producing enterobacter cloacae and their correlation with clinical outcome. J Clin Microbiol. 2009; 47(11): 3514-3519.
- Chen J, Allel, K, Zhuo, C, et al. Extended-Spectrum beta-lactamase-producing Escherichia coli and Klebsiella pneumoniae: risk factors and economic burden among patients with bloodstream infections. Risk Manag Healthc Policy. 2024; 17: 375-385.
- Macesic N, Hawkey, J, Vezina, B, et al. Genomic dissection of endemic carbapenem resistance reveals metallo-beta-lactamase dissemination through clonal, plasmid and integron transfer. Nat Commun. 2023; 14(1): 4764.
- Mostaghimi T, Shirafkan H, Nasrollahian S, et al. Worldwide prevalence of extended-spectrum β-lactamases-producing uropathogenic Escherichia coli isolates among kidney transplant patients: a systematic review and meta-analysis. Infez Med. 2023; 31(4): 466-475.
- Nasrollahian S, Halaji M, Hosseini A, et al. Genetic diversity, carbapenem resistance genes, and biofilm formation in UPEC isolated from patients with catheter-associated urinary tract infection in North of Iran. Int J Clin Pract. 2022; 2022: 9520362.
- Nasrollahian S, Graham JP, Halaji M. A review of the mechanisms that confer antibiotic resistance in pathotypes of E. coli. Front Cell Infect Microbiol. 2024; 14: 1387497.
- Falcone M, Russo, A, Iacovelli, A, et al. Predictors of outcome in ICU patients with septic shock caused by Klebsiella pneumoniae carbapenemase-producing K. pneumoniae. Clin Microbiol Infect. 2016; 22: 444-450.
- Falcone M, Giordano, C, Barnini, S, et al. Extremely drug-resistant NDM-9-producing ST147 Klebsiella pneumoniae causing infections in Italy, May 2020. Euro Surveill. 2020; 25(48).
- Tiseo G, Falcone, M, Leonildi, A, et al. Meropenem-vaborbactam as salvage therapy for ceftazidime-avibactam-, cefiderocol-resistant ST-512 Klebsiella pneumoniae-producing KPC-31, a D179Y Variant of KPC-3. Open Forum Infect Dis. 2021; 8(6): ofab141.
- Estabrook M, Muyldermans, A, Sahm, D, et al. Epidemiology of resistance determinants identified in meropenem-nonsusceptible enterobacterales collected as part of a global surveillance study, 2018 to 2019. Antimicrob Agents Chemother. 2023; 67(5): e0140622.
- Sader HS, Mendes, RE, Carvalhaes, CG, et al. Changing epidemiology of carbapenemases among carbapenem-resistant enterobacterales from united states hospitals and the activity of aztreonam-avibactam against contemporary Enterobacterales (2019-2021). Open Forum Infect Dis. 2023; 10: ofad046.
- Lorenzin G, Gona, F, Battaglia, S, et al. Detection of NDM-1/5 and OXA-48 co-producing extensively drug-resistant hypervirulent Klebsiella pneumoniae in Northern Italy. J Glob Antimicrob Resist. 2022; 28: 146-150.
- Mileto I, Petazzoni, G, Corbella, M, et al. Rapid spread of a novel NDM-producing clone of Klebsiella pneumoniae CC147, Northern Italy, February to August 2023. Euro Surveill. 2023; 28(42): 2300522.
- Tavoschi L, Forni, S, Porretta, A, et al. Prolonged outbreak of New Delhi metallo-beta-lactamase-producing carbapenem-resistant Enterobacterales (NDM-CRE), Tuscany, Italy, 2018 to 2019. Euro Surveill. 2020; 25(6): 2000085.
- ECDC. Rapid risk assessment - Carbapenem-resistant Enterobacterales – third update 2025. https://www.ecdc.europa.eu/en/publications-data/carbapenem-resistant-enterobacterales-rapid-risk-assessment-third-update (Accessed 19 May 2025).
- Falcone M, Tiseo, G, Antonelli, A, et al. Clinical features and outcomes of bloodstream infections caused by New Delhi metallo-beta-lactamase-producing Enterobacterales during a regional outbreak. Open Forum Infect Dis. 2020; 7: ofaa011.
- Di Pilato V, Henrici De Angelis, L, Aiezza, N, et al. Resistome and virulome accretion in an NDM-1-producing ST147 sublineage of Klebsiella pneumoniae associated with an outbreak in Tuscany, Italy: a genotypic and phenotypic characterisation. Lancet Microbe. 2022; 3(3): e224-e234.
- Loconsole D, Sallustio, A, Sacco, D, et al. Genomic surveillance of carbapenem-resistant Klebsiella pneumoniae reveals a prolonged outbreak of extensively drug-resistant ST147 NDM-1 during the COVID-19 pandemic in the Apulia region (Southern Italy). J Glob Antimicrob Resist. 2024; 36: 260-266.
- Falcone M, Tiseo, G, Arcari, G, et al. Spread of hypervirulent multidrug-resistant ST147 Klebsiella pneumoniae in patients with severe COVID-19: an observational study from Italy, 2020-21. J Antimicrob Chemother. 2022; 77(4): 1140-1145.
- Ben Nasr A, Decre, D, Compain, F, et al. Emergence of NDM-1 in association with OXA-48 in Klebsiella pneumoniae from Tunisia. Antimicrob Agents Chemother. 2013; 57(8): 4089-4090.
- Rotondo C, Venditti C, Butera O, et al. Molecular characterization of multidrug-resistant and hypervirulent New Delhi Metallo-Beta-Lactamase Klebsiella pneumoniae in Lazio, Italy: a five-year retrospective study. Antibiotics (Basel). 2024; 13(11): 1045.
- Di Marcantonio S, Perilli, M, Alloggia, G, et al. Coexistence of bla(NDM-5), bla(CTX-M-15), bla(OXA-232), bla(SHV-182) genes in multidrug-resistant K. pneumoniae ST437-carrying OmpK36 and OmpK37 porin mutations: First report in Italy. J Glob Antimicrob Resist. 2024; 37: 24-27.
- Gona F, Bongiorno D, Aprile A, et al. Emergence of two novel sequence types (3366 and 3367) NDM-1- and OXA-48-co-producing K. pneumoniae in Italy. Eur J Clin Microbiol Infect Dis. 2019; 38(9): 1687-1691.
- Posteraro B, De Maio, F, Motro, Y, et al. In-depth characterization of multidrug-resistant NDM-1 and KPC-3 co-producing Klebsiella pneumoniae bloodstream isolates from Italian hospital patients. Microbiol Spectr. 2024; 12(4): e0330523.
- Nicitra E, Terrana, M, Bongiorno, D, et al. Circulation of a unique Klebsiella pneumoniae clone, ST147 NDM-1/OXA-48, in two diverse hospitals in Calabria (Italy). Antibiotics (Basel). 2025; 14: 128.
- Fu B, Xu, J, Yin, D, et al. Transmission of bla (NDM) in Enterobacteriaceae among animals, food and human. Emerg Microbes Infect. 2024; 13(1): 2337678.
- Falcone M, Perilli M, Mezzatesta ML, et al. Prolonged bacteraemia caused by VIM-1 metallo-beta-lactamase-producing Proteus mirabilis: first report from Italy. Clin Microbiol Infect. 2010; 16(2): 179-181.
- Arcari G, Di Lella FM, Bibbolino G, et al. A multispecies cluster of VIM-1 carbapenemase-producing enterobacterales linked by a novel, highly conjugative, and broad-host-range inca plasmid forebodes the reemergence of VIM-1. Antimicrob Agents Chemother. 2020; 64(4): e02435-19.
- Olivieri R, Riccobono E, Gonnelli S, et al. Large, protracted, multi-species and multi-clonal spread of VIM-type metallo-β-lactamase-producing Enterobacterales in an Italian hospital. J Hosp Infect. 2025; 157: 10-18.
- Hagiya H, Yamamoto N, Kawahara R, et al. Risk factors for fecal carriage of IMP-6-producing Enterobacteriaceae at a long-term care hospital in Japan: a follow-up report from the Northern Osaka multicentre study group. J Infect Chemother. 2018; 24(9): 769-772.
- Falcone M, Tiseo G, Dentali F, et al. Predicting resistant etiology in hospitalized patients with blood cultures positive for Gram-negative bacilli. Eur J Intern Med. 2018; 53: 21-28.
- Falcone M, Paul M, Yahav D, et al. Antimicrobial consumption and impact of antimicrobial stewardship programmes in long-term care facilities. Clin Microbiol Infect. 2019; 25(5): 562-569.
- Falcone M, Russo A, Gentiloni Silverj F, et al. Predictors of mortality in nursing-home residents with pneumonia: a multicentre study. Clin Microbiol Infect. 2018; 24: 72-77.
- Falcone M, Tiseo, G, Galfo, V, et al. Bloodstream infections in patients with rectal colonization by Klebsiella pneumoniae producing different type of carbapenemases: a prospective, cohort study (CHIMERA study). Clin Microbiol Infect. 2022; 28: 298 e1- e7.
- Maugeri G, Calvo, M, Bongiorno, D, et al. Sequencing analysis of invasive carbapenem-resistant Klebsiella pneumoniae isolates secondary to gastrointestinal colonization. Microorganisms. 2025; 13(1): 89.
- Arzilli G, Scardina G, Casigliani V, et al. Screening for antimicrobial-resistant Gram-negative bacteria in hospitalised patients, and risk of progression from colonisation to infection: Systematic review. J Infect. 2022; 84(2): 119-130.
- Meini S, Del Cesta R, Sbrana F, et al. Clinical outcomes of patients hospitalized in internal medicine wards adequately treated for bloodstream infections caused by NDM-producing Klebsiella pneumoniae. Results from a real-life retrospective multi-center study in an endemic area. Infection. 2025 Mar 7. Epub ahead of print. Erratum in: Infection. 2025 Mar 18.
- Giuliano G, Hankache G, Sambo M, et al. Urinary tract infections caused by Gram-negative bacteria in elderly hospitalized patients: epidemiology, clinical features and outcomes in the era of antimicrobial resistance. J Glob Antimicrob Resist. 2025; 44: 116-126.
- De Pascale G, Cortegiani, A, Rinaldi, M, et al. Incidence of hospital-acquired infections due to carbapenem-resistant Enterobacterales and Pseudomonas aeruginosa in critically ill patients in Italy: a multicentre prospective cohort study. Crit Care. 2025; 29(1): 32.
- Dickstein Y, Yahav D, Tiseo, G, et al. Carbapenemase type and mortality in blood-stream infections caused by carbapenemase-producing enterobacterales: a multicenter retrospective cohort study. Infection 2025 Jun 16. Epub ahead of print.
- Falcone M, Bassetti, M, Tiseo, G, et al. Time to appropriate antibiotic therapy is a predictor of outcome in patients with bloodstream infection caused by KPC-producing Klebsiella pneumoniae. Crit Care. 2020; 24(1): 29.
- Metan G, Akova, M. Reducing the impact of carbapenem-resistant Enterobacteriaceae on vulnerable patient groups: what can be done? Curr Opin Infect Dis. 2016; 29(6): 555-560.
- Zhuang Q, Guo, H, Peng, T, et al. Advances in the detection of beta-lactamase: a review. Int J Biol Macromol. 2023; 251: 126159.
- Bianco G, Boattini M, van Asten SAV, et al. RESIST-5 O.O.K.N.V. and NG-Test Carba 5 assays for the rapid detection of carbapenemase-producing Enterobacterales from positive blood cultures: a comparative study. J Hosp Infect. 2020; 105(2): 162-166.
- Wang Y, Song, H, Xu, M, et al. Comparing the broth enrichment-multiplex lateral flow immunochromatographic assay with real time quantitative PCR for the rapid detection of carbapenemase-producing organisms in rectal swabs. BMC Infect Dis. 2023; 23(1): 413.
- Stokes W, Pitout, J, Campbell, L, et al. Rapid detection of carbapenemase-producing organisms directly from blood cultures positive for Gram-negative bacilli. Eur J Clin Microbiol Infect Dis. 2021; 40(2): 381-384.
- CLSI M100 Performance Standards for Antimicrobial Susceptibility Testing. 27th Jan 2025. Available at: https://clsi.org/shop/standards/m100/. Last access on 19th Aug 2025.
- EUCAST. RAST: Screening for resistance mechanisms of epidemiological and/or infection control importance. 18th March 2025. Available at: https://www.eucast.org/screening_for_resistance_mechanisms_with_rast. Last access on 19th Aug 2025.
- Sullivan E, Macias Jimenez MD, Moore NM. Utilization of an immunochromatographic lateral flow assay for rapid detection of carbapenemase production in gram negative bacilli. Lab Med. 2023; 54(6): e204-e206.
- Sangiorgio G, Calvo, M, Stefani, S. Aztreonam and avibactam combination therapy for metallo-beta-lactamase-producing gram-negative bacteria: a Narrative Review. Clin Microbiol Infect. 2025; 31(6): 971-978.
- Bai Y, Hao, Y, Shao, C, et al. Accuracy of Xpert Carba-R assay for the diagnosis of carbapenemase-producing organisms from rectal swabs and clinical isolates: a meta-analysis of diagnostic studies. J Mol Diagn. 2021; 23(11): 1534-1544.
- WHO. 2023 Antibacterial agents in clinical and preclinical development: an overview and analysis 2024. Available at: https://www.who.int/publications/i/item/9789240094000. Last access on 6th June 2025.
- Bassetti M, Larosa, B, Vena, A, et al. Novel agents in development for the treatment of resistant Gram-negative infections. Expert Rev Anti Infect Ther. 2024; 22(11): 965-976.
- Coppi M, Antonelli A, Niccolai C, et al. Nosocomial outbreak by NDM-1-producing Klebsiella pneumoniae highly resistant to cefiderocol, Florence, Italy, August 2021 to June 2022. Euro Surveill. 2022; 27(43): 2200795.
- Tascini C, Coppi, M, Antonelli, A, et al. In vivo evolution to high-level cefiderocol resistance of NDM-1-producing Klebsiella pneumoniae, followed by intra-hospital cross-transmission. Clin Microbiol Infect. 2024; 30(3): 398-400.
- Russo A, Bruni A, Gulli S, et al. Efficacy of cefiderocol- vs colistin-containing regimen for treatment of bacteraemic ventilator-associated pneumonia caused by carbapenem-resistant Acinetobacter baumannii in patients with COVID-19. Int J Antimicrob Agents. 2023; 62(1): 106825.
- Falcone M, Tiseo, G. Cefiderocol for the treatment of metallo-beta-lactamases producing Gram-negative bacilli: lights and shadows from the literature. Clin Infect Dis. 2022; 75(6): 1085-1087.
- Karakonstantis S, Rousaki M, Vassilopoulou L, Kritsotakis EI. Global prevalence of cefiderocol non-susceptibility in Enterobacterales, Pseudomonas aeruginosa, Acinetobacter baumannii, and Stenotrophomonas maltophilia: a systematic review and meta-analysis. Clin Microbiol Infect. 2024; 30: 178-188.
- Russo C, Mesini, A, Mariani, M, et al. Reduce susceptibility to cefiderocol in Gram negative bacteria in children: is hope already lost before it’s even arrived? J Infect Public Health. 2024; 17(4): 624-631.
- EMA. New antibiotic to fight infections caused by multidrug-resistant bacteria 2024. Available at: https://www.ema.europa.eu/en/news/new-antibiotic-fight-infections-caused-multidrug-resistant-bacteria. Last accessed 10 June 2025.
- Falcone M, Menichetti, F, Cattaneo, D, et al. Pragmatic options for dose optimization of ceftazidime/avibactam with aztreonam in complex patients. J Antimicrob Chemother. 2021; 76(4): 1025-1031.
- Falcone M, Daikos, GL, Tiseo, G, et al. Efficacy of ceftazidime-avibactam plus aztreonam in patients with bloodstream infections caused by metallo-beta-lactamase-producing Enterobacterales. Clin Infect Dis. 2021; 72(11): 1871-1878.
- Meschiari M, Asquier-Khati, A, Tiseo, G, et al. Treatment of infections caused by multidrug-resistant Gram-negative bacilli: a practical approach by the Italian (SIMIT) and French (SPILF) Societies of Infectious Diseases. Int J Antimicrob Agents. 2024; 64(1): 107186.
- Tiseo G, Brigante, G, Giacobbe, DR, et al. Diagnosis and management of infections caused by multidrug-resistant bacteria: guideline endorsed by the Italian Society of Infection and Tropical Diseases (SIMIT), the Italian Society of Anti-Infective Therapy (SITA), the Italian Group for Antimicrobial Stewardship (GISA), the Italian Association of Clinical Microbiologists (AMCLI) and the Italian Society of Microbiology (SIM). Int J Antimicrob Agents. 2022; 60(2): 106611.
- Salvia T, Dolma KG, Dhakal OP, et al. Phenotypic Detection of ESBL, AmpC, MBL, and Their Co-occurrence among MDR Enterobacteriaceae Isolates. J Lab Physicians. 2022; 14(3): 329-335.
- Rossolini GM, Arhin, FF, Kantecki, M. In vitro activity of aztreonam-avibactam and comparators against metallo-beta-Lactamase-producing Enterobacterales from ATLAS Global Surveillance Program, 2016-2020. Glob Antimicrob Resist. 2024; 36: 123-131.
- Sader HS, Kimbrough JH, Mendes RE, et al. Antimicrobial susceptibility of enterobacterales causing bloodstream infection in United States medical centres: comparison of aztreonam-avibactam with beta-lactams active against carbapenem-resistant enterobacterales. BMC Infect Dis. 2024; 24(1): 1242.
- Sader HS, Mendes RE, Ryan Arends SJ, et al. Activity of aztreonam-avibactam and other beta-lactamase inhibitor combinations against Gram-negative bacteria isolated from patients hospitalized with pneumonia in United States medical centers (2020-2022). BMC Pulm Med. 2025; 25(1): 38.
- Santerre Henriksen A, Arena F, Attwood M, et al. In vitro activity of cefiderocol against European Enterobacterales, including isolates resistant to meropenem and recentbeta-lactam/beta-lactamase inhibitor combinations. Microbiol Spectr. 2024; 12(8): e0418123.
- Hamrick JC, Docquier JD, Uehara T, et al. VNRX-5133 (Taniborbactam), a broad-spectrum inhibitor of serine- and metallo-beta-lactamases, restores activity of cefepime in Enterobacterales and Pseudomonas aeruginosa. Antimicrob Agents Chemother. 2020; 64: e01963-e01919.
- Marchetti VM, Bitar I, Sarti M, et al. Genomic Characterization of VIM and MCR co-producers: the first two clinical cases, in Italy. Diagnostics (Basel). 2021; 11(1): 79.
- Tiseo G, Suardi, LR, Leonildi, A, et al. Meropenem/vaborbactam plus aztreonam for the treatment of New Delhi metallo-beta-lactamase-producing Klebsiella pneumoniae infections. J Antimicrob Chemother. 2023; 78(9): 2377-2379.
- Sawa T, Kooguchi, K, Moriyama, K. Molecular diversity of extended-spectrum beta-lactamases and carbapenemases, and antimicrobial resistance. J Intensive Care. 2020; 8: 13.