Le Infezioni in Medicina, n. 2, 190-202, 2025
doi: 10.53854/liim-3302-5
ORIGINAL ARTICLES
Self-perceived stigma in people living with HIV in Spain: a mixed-methods study
Yelson Alejandro Picón-Jaimes1, Ivan David Lozada-Martínez2, Mar Rosàs Tosas1, Juan Tiraboschi3
1Blanquerna-School of Health Sciences- Ramon Llull University, Barcelona, Spain;
2Biomedical Scientometrics and Evidence-Based Research Unit, Department of Health Sciences, Universidad de la Costa, Barranquilla, Colombia;
3Infectious Diseases Service -Bellvitge-IDIBELL-University Hospital-University of Barcelona, Hospitalet de Llobregat, Spain.
Article received 18 February 2025 and accepted 18 April 2025
Corresponding author
Yelson Alejandro Picón-Jaimes
E-mail: yelsonalejandropj@blanquerna.url.edu
SummaRY
Introduction: Despite medical advances, stigma against people living with HIV remains a major issue, especially in healthcare. Factors like ignorance and lack of training contribute to discrimination; studies show stigma varies by setting and provider background. This study in Spain aimed to explore self-perceived stigma and its impact on healthcare access.
Methods: This mixed-methods study in Spain assessed self-perceived stigma among people living with HIV using a validated questionnaire and semi-structured interviews. Participants were recruited via social media and public announcements. Data analysis involved statistical tests and qualitative coding. Ethical approval was obtained, ensuring confidentiality and compliance with European regulations.
Results: The study included 525 participants, mostly men (53.3%), with a median age of 38 years and an average of four years since diagnosis. The majority (96.2%) received care through the public healthcare system.
Stigma levels varied; internalised stigma was low, with most rejecting negative feelings about living with HIV. However, anticipated and experienced stigma remained, particularly in healthcare settings, where many reported discrimination and neglect—findings corroborated in interviews. Avoiding physical contact with patients and the excessive use of barrier measures were common behaviours. Analysis showed that stigma decreases with age and time since diagnosis but is higher among non-binary individuals.
Conclusions: This study highlighted varying levels of stigma affecting people living with HIV, particularly in healthcare. While internalised stigma was low, many anticipated or experienced discrimination, often due to impersonal treatment and unfounded fears, emphasising the need for education and awareness to foster respectful, empathetic care.
Keywords: HIV infections, social stigma, attitude of health personnel, psychosocial impact, physician-patient relations.
INTRODUCTION
Four decades since the first documented HIV case in 1981, stigma against people living with HIV (PLWH) remains entrenched, particularly in healthcare environments where compassionate care should prevail [1-3]. This enduring stigma, perpetuated by persistent misinformation and unfounded prejudice, systematically compromises both clinical care standards and patients’ psychosocial wellbeing. Although antiretroviral therapy has rendered HIV a medically controllable chronic condition, profound sociocultural barriers continue to hinder progress in the global HIV response [4, 5].
Research confirms stigma’s persistence across contexts, with prevalence varying by setting and provider type. A systematic review identify higher stigma among white male primary care physicians lacking HIV training [6]. Discriminatory attitudes correlate with gender, race, religion and clinical environment, often rooted in historical stereotypes of PLWH [6, 7]. However, in settings with policies aimed at reducing stigma, its impact is significantly lower [8].
A Laotian study of 558 healthcare workers found 45.7% maintained stigmatising attitudes despite 50% having HIV training and adequate knowledge [9]. Notably, clinicians with more PLWH experience and better training exhibited fewer discriminatory views, underscoring how knowledge gaps sustain stigma [9].
In Europe, stigma remains a major barrier to healthcare access, rights protection, and social support for PLWH. Within healthcare settings, many PLWH face discrimination, such as denial of treatment or disclosure of their HIV status without consent, leading to fear and delays in seeking medical care [10, 11]. To address this issue, strategies such as healthcare professional training, media campaigns, and telemedicine to improve patient privacy have been implemented. However, further efforts and resources are still required to ensure an effective reduction in stigma across the region [10, 11].
Critically, PLWH’s subjective healthcare experiences reveal stigma manifesting as verbal abuse, social exclusion and physical threats [12, 13]. Fear of discrimination deters status disclosure, complicating treatment access and potentially triggering treatment abandonment, relationship breakdowns and mental health crises [12, 13]. For this reason, we conducted a mixed-methods study in Spain to assess self-perceived stigma among PLWH. Combining quantitative and qualitative approaches, we aimed to document lived experiences of stigma and its healthcare access implications. Beyond mapping the problem, this research provides evidence to inform targeted stigma-reduction strategies in clinical settings.
METHODS
Study design
An observational, descriptive, and cross-sectional study was conducted, applying a validated questionnaire to PLWH, complemented by semi-structured interviews, thereby obtaining an explanatory model [14]. The study adhered to STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) and COREQ (Consolidated Criteria for Reporting Qualitative Research) guidelines.
Context
In Spain, HIV care is delivered through a decentralised, publicly funded National Health System, with private options also available. Patients are mainly treated in multidisciplinary hospital units by internal medicine or specially trained family physicians, as infectious disease is not a formal medical specialty. Although continuity with the same doctor varies, care is generally provided by a consistent team of specialists.
Recruitment was conducted across multiple healthcare service levels, with participants primarily recruited from public hospital settings. A smaller proportion were recruited from private hospitals and both public and private primary care centres. This distribution corresponds to the specialised nature of HIV treatment in Spain, where most patients receive care in hospital-based units rather than primary care settings.
Data collection took place in 2024 using an online questionnaire, ensuring confidentiality and data protection in compliance with European regulations. The instrument’s wording was culturally adapted for optimal comprehension by the Spanish population, though no additional questions were added or modified in content. A pilot test with 20 volunteers was conducted to verify the questionnaire’s clarity and cultural appropriateness.
Participants
Individuals aged 18 or older, living with HIV, receiving healthcare in Spain, and voluntarily providing informed consent were included. Those not residing in Spain, as well as travellers, students with stays shorter than six months, and migrants in transit, were excluded.
Recruitment and data sources
Given the sensitivity of the topic and the challenges of engaging populations affected by HIV-related stigma, a non-probabilistic purposive sampling method was deemed most appropriate. To broaden participation while safeguarding confidentiality, a snowball sampling approach was employed, enabling participants to refer others with shared experiences. However, recognising the potential for selection bias - particularly the risk of overrepresentation within close-knit networks - recruitment strategies were deliberately diversified to capture a wider spectrum of perspectives.
Initial outreach was conducted through multiple channels to engage diverse subgroups. A dedicated Instagram account (@Stopstigma_hiv) was established to collaborate with non-governmental organisations (NGOs) across different regions and communities, facilitating questionnaire distribution via direct links and QR codes. Efforts were extended to Facebook and LinkedIn to reach broader audiences. Additionally, the study was promoted through the #HiloTesis academic contest on X (formerly Twitter), ensuring the inclusion of participants with varying levels of experience regarding stigma toward PLWH.
To mitigate the inherent biases of snowball sampling, the initial “seed” participants were strategically selected from distinct networks, including healthcare providers living with HIV, LGBTQ+ activists, and peer support groups, thereby reducing reliance on a single demographic. While this approach enhanced the diversity of self-perceived stigma levels represented, we acknowledge that the sample may not fully reflect the broader population due to the non-randomised recruitment process.
Variables
Sociodemographic data (gender, age, education level, autonomous community, and type of healthcare service) and clinical data (time since HIV diagnosis) were collected. Self-perceived stigma was measured using the validated questionnaire by Earnshaw et al., consisting of 25 Likert-scale items assessing internalised stigma (α=0.89), anticipated stigma (α=0.87), and enacted stigma (α=0.87) [14].
Bias
Non-probabilistic sampling and the snowball method may introduce selection and response biases, limiting representativeness and potentially overestimating stigma prevalence. To mitigate these biases, the strategies previously described in the “Recruitment and Data Sources” section were employed.
Data analysis
Statistical analyses were performed using IBM SPSS v29. A univariate analysis was conducted using descriptive measures (mean, median, and standard deviation or interquartile range). To assess relationships between categorical variables, contingency tables with absolute and relative frequencies were used.
Since the data did not follow a normal distribution, non-parametric tests such as Kruskal-Wallis were applied to compare stigma levels across gender, education level, province of residence, and type of healthcare service, considering differences significant at p<0.05. Post hoc comparisons were performed using the Wilcoxon test.
A correlation matrix using Spearman’s Rho coefficient was employed to examine the relationships between age, time since diagnosis, and the three types of stigma.
Qualitative phase
The principal investigator, a physician with training in bioethics and HIV, conducted the interviews. A phenomenological approach was used to explore the subjective experiences of PLWH. Participants were selected through the questionnaire on social media, where an open-ended question allowed those interested to provide their email addresses.
Interviews were conducted virtually, with an audio-only option to preserve privacy. Recording was authorised, and data were analysed using ATLAS.ti 24. Two researchers independently coded the data, structuring them into inductively derived thematic categories.
Interviews lasted between 40 and 60 minutes and were conducted until data saturation was reached. Full transcripts were not returned to participants, but key points were verified during the interviews. A formal respondent validation of findings was not conducted; however, verbatim quotes with unique codes were included to illustrate themes.
Whilst all interviews were conducted by the principal investigator to ensure consistency in data collection, several measures were implemented to mitigate potential interviewer bias:
1) The semi-structured interview guide was rigorously developed through consultation with three qualitative methodology experts and piloted beforehand;
2) Questions were phrased in open-ended, non-leading formats to minimise interpretive influence;
3) Two independent researchers analysed the raw data using ATLAS.ti 24, with inter-coder reliability assessed through regular consensus meetings;
4) Emerging themes were systematically compared against the original transcripts to verify they reflected participants’ accounts rather than researchers’ assumptions.
Ethical considerations
The study complied with the principles of the Declaration of Helsinki and European data protection regulations (Regulation 2016/679). Informed consent was obtained from participants, and the study received approval from the Clinical Research Ethics Committee of Hospital de Bellvitge in Catalonia (Act 03/24, Ref. PR352/23).
RESULTS
Quantitative Phase
Following the dissemination of the study via social media and scientific events, it was estimated that 4,000 people accessed the call for participation. Of these, 525 responded to the questionnaire, resulting in a response rate of 13.1%.
Sociodemographic Characteristics
The majority of participants were male (53.3%), with a median age of 38 years (IQR: 19) and a median time since HIV diagnosis of 4 years (IQR: 4). The sample consisted predominantly of individuals identifying as heterosexual (61.0%, n=320) and homosexual (23.8%, n=125), with the remainder comprising those identifying as bisexual or who declined to state their orientation. Regarding educational attainment, 32.4% had technical qualifications, 25.7% held university degrees, and 14.1% had secondary education. Nearly all participants (96.2%) received care through the public health system, with 95.2% treated in public hospitals. Complete data are presented in Table 1 and Figure 1.
Table 1 - Characteristics of the participants.
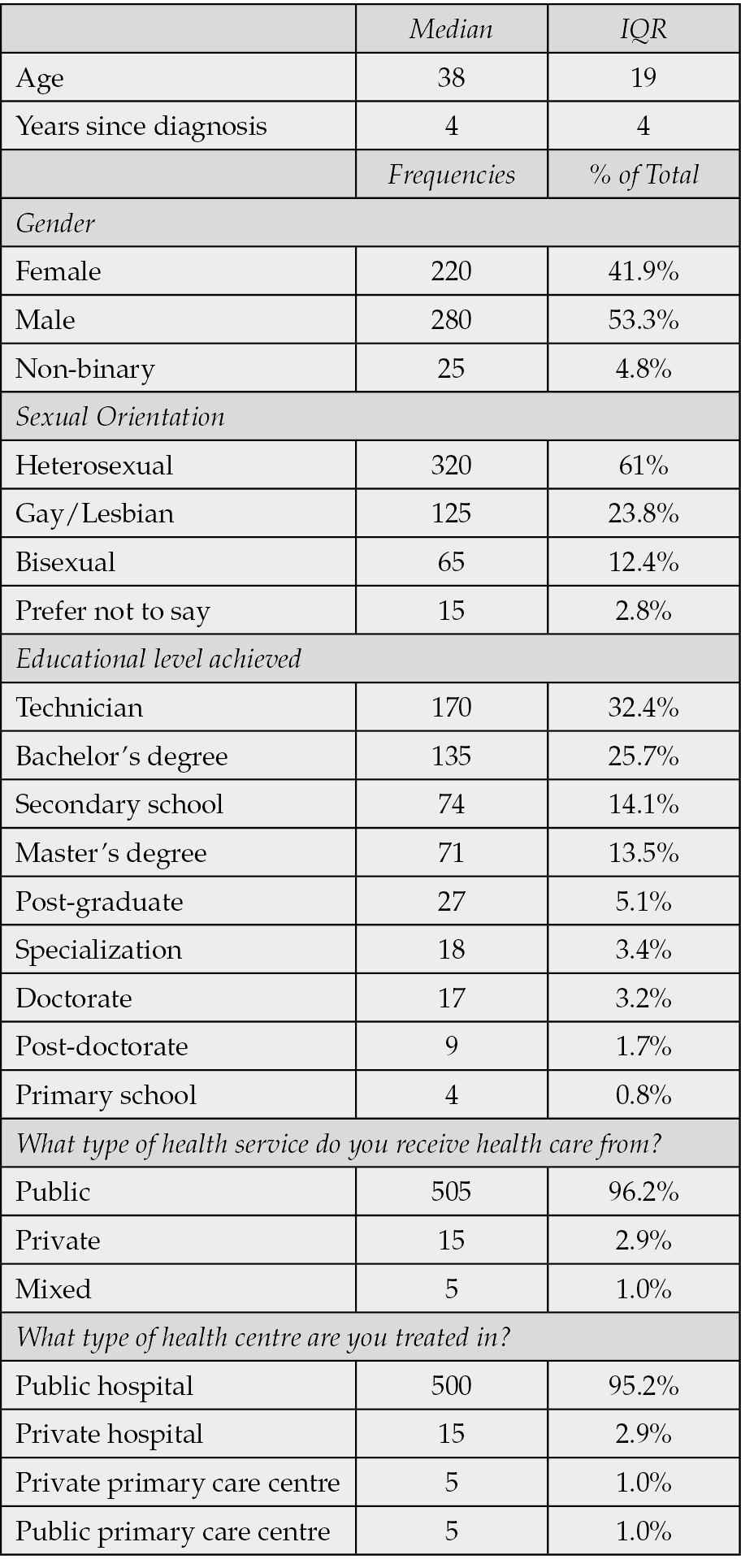

Figure 1 - Geographical distribution of participants.
Levels of self-perceived stigma in each dimension Internalised stigma
The majority of participants rejected stigmatising ideas associated with living with HIV. A total of 72.2% strongly disagreed that their diagnosis made them feel like a bad person, and 71.8% rejected the idea of not being as good as others.
Shame associated with the diagnosis had little acceptance, with 65.9% strongly disagreeing with feeling ashamed, and only 3.2% stating that they felt shame for being a PLWH. Similarly, most participants rejected the association of HIV with thoughts of impurity or repulsion (79.4% and 78.9%, respectively). Table 2 provides a detailed breakdown of responses related to internalised stigma.
Table 2 - Internalised stigma.

Anticipated stigma
The perception of stigma within family and healthcare environments varied among participants. In the family setting, just over half considered it unlikely that they would be avoided (51.0%) or looked down upon (50.9%), although a third remained undecided. A total of 24.4% believed it was possible that they would be treated differently by their family, while 43.2% had no clear stance on the matter.
Within the healthcare context, uncertainty was predominant. Nearly half were unsure whether professionals would take their needs seriously (49.7%), discriminate against them (60.8%), or avoid touching them (49.7%). However, 20.2% believed their needs would not be adequately addressed, and 17.3% anticipated that healthcare professionals would avoid physical contact.
Although most did not consider discrimination likely, doubts and concerns about stigma in healthcare settings persisted. Table 3 presents the full responses.
Table 3 - Anticipated stigma.

Experienced stigma
A significant proportion of participants experienced some degree of discrimination within both family and healthcare environments. In the family setting, the majority reported that they were rarely or never avoided (46.5% and 29.0%) or looked down upon (44.6% and 29.9%). However, 56.6% indicated that they had been treated differently on at least one occasion, while 16% stated that this occurred frequently.
In healthcare settings, 53.9% reported that their needs were not taken seriously on some occasions, and 20.8% experienced this often. Additionally, 35.6% stated that they had been discriminated against at least once, while 31.0% had never encountered such treatment. A total of 59.0% felt that their concerns were not listened to on some occasions, with 21.5% reporting that this happened frequently.
Physical contact was also a relevant issue, with 49.0% perceiving avoidance by healthcare staff on some occasions and 27.5% experiencing this frequently. In contrast, disrespectful treatment was less common, as 64.6% reported experiencing it rarely, and 19.6% stated that they had never encountered it.
Although stigma was not a universal experience, many participants faced differential treatment. Table 4 presents the full responses.
Table 4 - Experienced stigma.

Reliability of the Questionnaire
Cronbach’s α and McDonald’s ω values exceeded 0.85 across all subscales, indicating high reliability of the instrument, similar to findings reported by Earnshaw et al. [14]. Table 5 presents these values.
Table 5 - Reliability analysis and descriptive statistics of the items of the questionnaire on stigma in PLWH.

Analysis and correlations regarding internalised, anticipated and experienced stigma
The Kruskal-Wallis’s test revealed significant differences in internalised (χ²=8.42, p=0.015), anticipated (χ²=8.59, p=0.01), and experienced stigma (χ²=8.39, p=0.015), although the effect size was small (ε²≈ 0.016).
Post hoc comparisons indicated that the “Non-Binary” group reported higher levels of stigma compared to the Female and Male groups (p<0.05 in all cases), with no significant differences observed between the latter two groups. The examination of stigma patterns by sexual orientation revealed statistically significant differences across all measured domains. Kruskal-Wallis tests demonstrated robust variation in internalised (χ²=9.17, p=0.011), anticipated (χ²=8.94, p=0.012), and experienced stigma (χ²=9.02, p=0.011), with small-to-moderate effect sizes (ε²≈ 0.021). Post hoc analyses identified three key patterns: firstly, gay and lesbian participants reported consistently elevated stigma levels, scoring 23-27% higher than their heterosexual counterparts across all domains (all p<0.01). Secondly, bisexual individuals exhibited particularly pronounced disparities in internalised stigma (mean difference=1.8 points, 95% CI [1.1, 2.5], p=0.007). Lastly, participants who declined to specify their orientation displayed intermediate values, reaching statistical significance only for anticipated stigma when compared to heterosexual respondents (p=0.032).
No significant differences were found concerning educational level, province of residence, or place of care; therefore, these analyses were not included.
Correlation between age, time since diagnosis, internalised stigma, anticipated stigma and experienced stigma
Age did not show a significant correlation with internalised stigma (Rho=0.006, p=0.896). However, it was negatively correlated with anticipated stigma (Rho=-0.348, p<0.001) and experienced stigma (Rho=-0.124, p=0.004), indicating that older individuals perceived lower levels of anticipated and experienced stigma.
The time since diagnosis showed a negative correlation with internalised stigma (Rho=-0.214, p<0.001), anticipated stigma (Rho=-0.272, p<0.001), and experienced stigma (Rho=-0.154, p<0.001), suggesting that as more time passed since diagnosis, perceived stigma levels decreased.
Anticipated stigma was positively correlated with internalised stigma (Rho=0.523, p<0.001). Likewise, experienced stigma showed a strong correlation with both anticipated stigma (Rho=0.737, p<0.001) and internalised stigma (Rho=0.574, p<0.001), indicating that those who perceive higher levels of anticipated and internalised stigma are also more likely to experience it in their daily lives.
Qualitative Phase
Interviews were conducted with ten PLWH to explore their experiences and perceptions of the stigma they face within healthcare settings. The following section presents the profiles of the participants (Figure 2).

Figure 2 - Participant profiles and time living with HIV.
Meaning of stigma
When asked about the meaning of stigma, participants provided clear and deeply emotional definitions. A business owner expressed:
“Stigma is like a shadow that follows me, constantly reminding me that I am different, that my life is no longer like everyone else’s.”
A university student added:
“It is the fear of being judged. Sometimes I feel like my life is on hold because I have to hide that I was diagnosed with HIV. It’s difficult to form connections with others.”
A single mother emphasised that stigma is a social judgement that affects not only her health but also her ability to interact with others.
Personal experiences of stigma
Experiences within healthcare settings were varied and revealing. A shopkeeper recounted:
“Every time I visit the doctor, I feel like just another case, not a person with emotions and needs. They don’t ask me how I’m doing, only whether I’ve been taking my medication as prescribed. Sometimes they don’t even touch me, they don’t examine me – they’re only interested in my viral load.”
A nurse, who is also a patient, shared a painful experience:
“I’ve seen some of my colleagues treat HIV patients with distance, as if they feared the disease was airborne. Sometimes I see them put on double gloves and whisper the diagnosis to other colleagues, signalling them to take extra precautions. On some occasions, they don’t even try to hide it – they avoid touching patients as much as possible or only use the tips of their fingers.”
A young part-time worker spoke about her anxiety before medical visits, saying:
“I’m afraid of being looked at differently when I mention my diagnosis, especially when I see my GP or go for blood tests. Once, a nurse about to draw my blood told me, ‘Don’t move! I don’t want to prick myself.’”
These narratives reflect a pattern of rejection and distrust, which have affected their emotional well-being and created feelings of insecurity when seeking healthcare.
Impact on the physician-patient relationship
Stigma has deeply affected the participants’ relationships with healthcare professionals. A graphic designer mentioned:
“I can’t fully open up to my doctor. There’s always a barrier preventing me from being honest. Sometimes I have doubts, particularly questions about sexuality, but I don’t feel comfortable asking. Since I use private healthcare, I don’t have a single-family doctor – they change frequently, which creates even more distance. Every time I mention my diagnosis, there’s an awkward silence, and the conversation becomes tense.”
A retired participant, with years of experience, reflected:
“Sometimes I’d rather not go to the doctor because I know there will be comments that upset me. I’ve lived with this diagnosis for many years, and I’ve learned to accept myself and have a near-normal life – I’m not willing to be judged. At times, healthcare professionals lack sensitivity in how they say things, and that angers me. I’d rather avoid that frustration altogether.”
On the other hand, a psychologist shared a positive experience:
“I once had a doctor who treated me with dignity and respect, which encouraged me to continue with my treatment. She was quite young – I think younger generations are especially aware and capable of showing empathy. Many old-fashioned taboos have been broken. I believe older professionals still cling to times when showing emotions was frowned upon.”
Factors contributing to stigma
Participants identified several factors that contribute to stigma. A business owner pointed to the lack of HIV education among healthcare professionals, stating:
“Many doctors seem unsure about how to treat someone living with HIV – that in itself is stigma. If I go to the doctor for another issue, they hesitate to prescribe medication, they freeze, and I see them searching online to check if it’s compatible with my treatment. I see them doubt themselves.”
A single mother added that negative stereotypes are deeply ingrained in society, affecting how professionals interact with patients. The graphic designer also highlighted the need to demystify HIV through awareness campaigns in hospitals, suggesting:
“Better education could change perceptions – not only among healthcare professionals but also within the general public. The visibility of HIV is particularly important, especially in these turbulent political times, where we are starting to see more rejection than in previous years.”
Strategies to address stigma
Participants agreed that there are effective strategies to tackle stigma. A nurse suggested implementing ongoing HIV training programmes for healthcare professionals:
“It’s essential that professionals understand what it means to live with HIV and not just focus on the disease.”
The young part-time worker proposed the creation of support groups within healthcare centres, where patients can share their experiences without fear of judgement. A computer technician also emphasised the importance of including patient testimonies in professional training, stating:
“It humanises the experience and helps eliminate prejudice, showing that PLWH are sons, daughters, siblings, parents – in short, we are just people like anyone else, yet we face rejection from an uninformed society.”
DISCUSSION
The findings of this study provide a detailed insight into the perceptions and experiences of stigma among PLWH. While most participants rejected stigmatising ideas about themselves, a significant proportion still faced uncertainty and differential treatment, particularly in family and healthcare settings. This highlights the persistence of stigma at various levels and its impact on the daily lives of PLWH, in line with reports by other authors [15, 16].
The impact of internalised stigma extends beyond the social and medical spheres. For example, it has been observed that this stigma reduces the likelihood that mothers will disclose their serological status to their children. Davtyan et al. [17], found that higher levels of internalised stigma are associated with a lower willingness to share this information, which hinders family communication and HIV education at home.
Additionally, studies have shown that higher levels of stigma predict poorer cognitive performance in PLWH, suggesting that reducing stigma could improve cognitive function [18]. Likewise, the relationship between internalised stigma and mental health is evident in the literature. A study by Thapinta et al., showed that individuals with major depressive disorder had higher internalised stigma scores compared to those with mild depression or no depression [19]. Specifically, significant differences were found in the realm of social relationships (p<0.05), which aligns with previous research highlighting the close relationship between stigma and depressive symptoms [20, 21].
Our findings on anticipated stigma revealed that in the family environment, many participants did not believe it likely that they would be avoided or belittled. However, in healthcare settings, a significant proportion remained uncertain about whether they would face discrimination, while a smaller number anticipated that professionals might avoid physical contact. In comparison, Meyer et al., reported that 30.7% of respondents experienced anticipated stigma, indicating fear of negative experiences when receiving healthcare due to their serological status [22].
Various studies have demonstrated a strong relationship between anticipated stigma, internalised stigma, and depressive symptoms in PLWH [23]. This expectation of discrimination not only reinforces negative beliefs about oneself but also significantly impacts mental health (p<0.001), establishing a bidirectional relationship between anticipated stigma and depression over time (p<0.05) [23-26].
Furthermore, anticipated stigma influences access to healthcare services, a study among young people found that those with low levels of anticipated stigma were more likely to get tested for HIV, regardless of prior experiences of discrimination in the healthcare system [27]. In contrast, those who perceived higher levels of anticipated stigma and greater experiences of discrimination were less likely to get tested, confirming that anticipated stigma is a significant barrier to medical care. Research has also shown that this type of stigma indirectly affects adherence to antiretroviral therapy, reinforcing the need to address its impact on the health of PLWH [27-29].
Regarding experienced stigma in healthcare settings, our findings indicate that around half of the participants felt their needs were not always taken seriously, while a similar proportion noted that healthcare professionals occasionally avoided physical contact. The interviews revealed experiences of rejection, distant or overly cautious treatment, and a lack of empathy, which often led to feelings of anxiety, distrust, and difficulty in communicating openly with medical staff.
Stigma in healthcare is a well-documented reality, in the U.S., a study found that 23% of Hispanics living with HIV experienced discrimination in healthcare, with higher rates in men (23%) than in women (18%) and in Black Hispanics (28%) compared to Whites (21%) [30]. This discrimination is associated with lower use of healthcare services (Odds Ratio [OR]=1.76), depressive symptoms (OR=1.48), and lower adherence to antiretroviral treatment (OR=1.41) [31]. Additionally, a relationship has been identified between self-disclosure of HIV status and increased experienced (Prevalence Ratio [PR]=11.0) and internalised (PR=2.3) stigma, especially among those who disclosed it to their family (PR=13.0) [32]. However, these people also tended to report milder depressive symptoms (PR=1.8), although the connection with moderate to severe symptoms was less clear [32].
Recent studies in developed countries have shown that stigma towards PLWH persists and is associated with psychological distress, lower social support, and poor adherence to treatment [33-36]. Nevertheless, testimonies in our study highlighted that empathetic and respectful treatment from some doctors can transform the patient experience. Combating stigma through education and sensitivity is key to ensuring dignified and accessible care. This is why efforts should be directed towards creating new strategies to improve the care of PLWH.
This mixed-methods study has some limitations, such as the study’s recruitment strategy may have introduced selection bias. Given the sensitive nature of HIV-related stigma, participants were likely to be those who had personally experienced stigmatisation or were actively engaged in advocacy work, potentially under-representing individuals who avoid disclosure due to fear of discrimination. Whilst the snowball sampling approach enhanced diversity by incorporating healthcare professionals, LGBTQ+ activists and peer support group members, the sample may not adequately represent more marginalised or digitally excluded populations. This limitation warrants consideration when interpreting the findings, as the results may overestimate the prevalence or intensity of self-perceived stigma within the broader population of PLWH.
Although the sample is representative, it is limited in size and context, which makes it difficult to generalise the findings. A further limitation arises from the study design’s lack of a control group, which prevents definitive attribution of the results specifically to being a PLWH. However, the alignment of our findings with existing evidence on HIV-related stigma supports their validity. Finally, while the qualitative methodology provides a deeper understanding, the results may not be extrapolatable to other populations with different sociocultural realities.
Our findings demonstrate the pressing need for comprehensive interventions to reduce stigma experienced by PLWH in healthcare settings. A key priority should involve mandatory training for healthcare staff, incorporating specific modules on non-stigmatising communication and implicit bias management within continuing professional development programmes, following models already validated in European healthcare systems. Additionally, evidence-based digital interventions could be developed, utilising first-person narratives from PLWH on high-impact platforms whose algorithms can effectively reach key populations. These proposals, aligned with UNAIDS objectives, could initially be implemented in autonomous communities with higher population density to assess effectiveness before nationwide rollout within the national health system.
CONCLUSIONS
This study revealed that PLWH experienced multi-layered stigma, particularly in healthcare settings, where impersonal treatment and transmission fears damage patient-provider relationships. While most participants did not internalize stigma, many encountered discriminations, with emotional disconnection from clinicians emerging as a critical concern. The analysis showed that stigma perceptions diminished over time post-diagnosis, suggesting long-term support fostered resilience. The findings highlighted the urgent need for clinician training and public awareness campaigns to humanize HIV care.
Whilst this study provides valuable insights into self-perceived stigma among PLWH, the recruitment methodology – relying primarily on social media and peer referrals – may have skewed the sample towards individuals more willing to disclose their status. This underscores the importance of developing more inclusive sampling strategies in future research.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
REFERENCES
[1] Picón-Jaimes YA, Lozada-Martínez ID, Tosàs MR, et al. Stigma and fear of getting sick in the care of people living with HIV: an exploratory systematic review. Infez Med. 2024; 32(2): 168-182.
[2] Cobos I, Jackson-Perry D, Courvoisier C, et al. Stigma and HIV: relevant for everyone. Rev Med Suisse. 2020; 16(690): 744-748.
[3] Restall G, Ukoli P, Mehta P, et al. Resisting and disrupting HIV-related stigma: a photovoice study. BMC Public Health. 2023; 23(1): e2062.
[4] Guilamo-Ramos V, Thimm-Kaiser M, Benzekri A. The U.S. Latino HIV Crisis - Ending an Era of Invisibility. N Engl J Med. 2024; 391(18): 1665-1668.
[5] Fauk NK, Hawke K, Mwanri L, et al. Stigma and Discrimination towards People Living with HIV in the Context of Families, Communities, and Healthcare Settings: A Qualitative Study in Indonesia. Int J Environ Res Public Health. 2021; 18(10): e5424.
[6] Geter A, Herron AR, Sutton MY. HIV-Related Stigma by Healthcare Providers in the United States: A Systematic Review. AIDS Patient Care STDs. 2018; 32(10): 418-424.
[7] Galal YS, Khairy WA, Mohamed R, et al. HIV-related stigma and discrimination by healthcare workers in Egypt. Trans R Soc Trop Med Hyg. 2022; 116(7): 636-644.
[8] Nyblade L, Stockton MA, Giger K, et al. Stigma in health facilities: why it matters and how we can change it. BMC Med. 2019; 17(1): e25.
[9] Vorasane S, Jimba M, Kikuchi K, et al. An investigation of stigmatizing attitudes towards people living with HIV/AIDS by doctors and nurses in Vientiane, Lao PDR. BMC Health Serv Res. 2017; 17(1): e125.
[10] Schweitzer AM, Dišković A, Krongauz V, et al. Addressing HIV stigma in healthcare, community, and legislative settings in Central and Eastern Europe. AIDS Res Ther. 2023; 20(1): e87.
[11] Vaughan E, Költő A. Drivers and Facilitators of HIV-Related Stigma in Healthcare Settings in Ireland. AIDS Behav. 2025; 29(1): 22-36.
[12] Jan S, Manzoor S, Rashid J. Experiences of stigma and discrimination of women living with HIV/AIDS in health-care settings of Kashmir. Indian J Public Health. 2023; 67(1): 155-158.
[13] Mohammed A, Cheabu BS, Amoah-Larbi J, et al. Perception and experience of HIV-induced stigma among people with HIV seeking healthcare in Ghana. BMC Health Serv Res. 2024; 24(1): e1449.
[14] Earnshaw VA, Smith LR, Chaudoir SR, et al. HIV stigma mechanisms and well-being among PLWH: a test of the HIV stigma framework. AIDS Behav. 2013; 17(5): 1785-1795.
[15] Ferguson L, Gruskin S, Bolshakova M, et al. Frameworks and measures for HIV-related internalized stigma, stigma and discrimination in healthcare and in laws and policies: a systematic review. J Int AIDS Soc. 2022; 25(Suppl. 1): e25915.
[16] Hempel S, Ferguson L, Bolshakova M, et al. Frameworks, measures, and interventions for HIV-related internalised stigma and stigma in healthcare and laws and policies: systematic review protocol. BMJ Open. 2021; 11(12): e053608.
[17] Davtyan M, Kacanek D, Lee J, et al. The role of internalised HIV stigma in disclosure of maternal HIV serostatus to children perinatally HIV-exposed but uninfected: a prospective study in the United States. J Int AIDS Soc. 2023; 26(Suppl. 4): e26167.
[18] Thompson EC, Muhammad JN, Adimora AA, et al. Internalized HIV-Related Stigma and Neurocognitive Functioning Among Women Living with HIV. AIDS Patient Care STDs. 2022; 36(9): 336-342.
[19] Thapinta D, Srithanaviboonchai K, Uthis P, et al. Association between Internalized Stigma and Depression among People Living with HIV in Thailand. Int J Environ Res Public Health. 2022; 19(8): e4471.
[20] Chan BT, Pradeep A, Prasad L, et al. Association between internalized stigma and depression among HIV-positive persons entering into care in Southern India. J Glob Health. 2017; 7(2): e020403.
[21] Kalomo EN. Associations between HIV-related stigma, self-esteem, social support, and depressive symptoms in Namibia. Aging Ment Health. 2018; 22(12): 1570-1576.
[22] Meyer MF, Moe CA, Galagan SR, et al. Symbolic and anticipated HIV stigma are associated with mental health and education in South Africa. AIDS Care. 2023; 35(11): 1700-1707.
[23] Yuan GF, Tam CC, Yang X, et al. Associations Between Internalized and Anticipated HIV Stigma and Depression Symptoms Among People Living with HIV in China: A four-wave Longitudinal Model. AIDS Behav. 2023; 27(12): 4052-4061.
[24] Dai Z, Fu J, Qu Y, et al. Depressive symptoms, perceived social support, and anticipated HIV stigma among HIV-negative/unknown men who have sex with men in China during the COVID-19 pandemic: A multicenter online cross-sectional study. Brain Behav. 2023; 13(4): e2946.
[25] Fu J, Chen X, Dai Z, et al. HIV-related stigma, depression and suicidal ideation among HIV-positive MSM in China: a moderated mediation model. BMC Public Health. 2023; 23(1): e2117.
[26] Yan H, Li X, Li J, et al. Association between perceived HIV stigma, social support, resilience, self-esteem, and depressive symptoms among HIV-positive men who have sex with men (MSM) in Nanjing, China. AIDS Care. 2019; 31(9): 1069-1076.
[27] D’Anna LH, Chang K. Healthcare discrimination, anticipated HIV stigma, and income as predictors of HIV testing among a community sample of YBMSM. AIDS Care. 2024; 36(2): 212-219.
[28] Zeng C, Li X, Qiao S, et al. Anticipated stigma and medication adherence among people living with HIV: the mechanistic roles of medication support and ART self-efficacy. AIDS Care. 2020; 32(8): 1014-1022.
[29] Yuan GF, Qiao S, Li X, et al. How Does Anticipated HIV Stigma Affect Medication Adherence? A Longitudinal Path Analysis Model. AIDS Behav. 2024; 28(5): 1684-93.
[30] Padilla M, Patel D, Beer L, et al. HIV Stigma and Health Care Discrimination Experienced by Hispanic or Latino Persons with HIV - United States, 2018-2020. MMWR Morb Mortal Wkly Rep. 2022; 71(41): 1293-1300.
[31] Friedman MR, Liu Q, Meanley S, et al. Biopsychosocial Health Outcomes and Experienced Intersectional Stigma in a Mixed HIV Serostatus Longitudinal Cohort of Aging Sexual Minority Men, United States, 2008-2019. Am J Public Health. 2022; 112(S4): 452-462.
[32] Mugo C, Seeh D, Guthrie B, et al. Association of experienced and internalized stigma with self-disclosure of HIV status by youth living with HIV. AIDS Behav. 2021; 25(7): 2084-2093.
[33] Drewes J, Langer PC, Ebert J, et al. Associations Between Experienced and Internalized HIV Stigma, Adversarial Growth, and Health Outcomes in a Nationwide Sample of People Aging with HIV in Germany. AIDS Behav. 2021; 25(4): 1037-1046.
[34] Dockerty C, Shannon K, Wechsberg W, et al. Stigma, Discrimination and Other Social-Structural Factors Associated with Barriers to Counselling or Therapy among Women Living with HIV Who have Experienced Violence in Metro Vancouver, Canada. AIDS Behav. 2024; 28(11): 3919-3928.
[35] Stutterheim SE, Kuijpers KJ, Waldén MI, et al. Trends in HIV Stigma Experienced by People Living With HIV in the Netherlands: A Comparison of Cross-Sectional Surveys Over Time. AIDS Educ Prev. 2022; 34(1): 33-52.
[36] Lo Hog Tian JM, Watson JR, Ibáñez-Carrasco F, et al. Impact of experienced HIV stigma on health is mediated by internalized stigma and depression: results from the people living with HIV stigma index in Ontario. BMC Public Health. 2021; 21(1): e1595.