Le Infezioni in Medicina, n. 1, 50-63, 2025
doi: 10.53854/liim-3301-5
REVIEWS
Dengue in patients with kidney transplant: a systematic review
Andres Felipe Salazar-Urbano1,2, Otto Alberto Sussmann-Peña1,2, Jonathan Alexander Guezguan-Perez3, Angie Alejandra Ortiz-Parra1,4, Jesika Lorena Cruz-Muñoz1,4, Karol Daniela Mosquera-Niño1,4, Luis Gabriel Reyes-Hernández1,4, Alfonso J. Rodriguez-Morales5,6
1Semillero de Investigación en Infectología Clínica, Infectoclínicos, SAS, Bogotá, DC, Colombia;
2Infectoclínicos, SAS, Bogotá, DC, Colombia;
3Subred Integrada de Servicios de Salud Centro Oriente, E.S.E. Hospital Santa Clara, Bogotá, DC, Colombia;
4Universidad Antonio Nariño, Bogotá, DC, Colombia;
5Masters’ Program of Clinical Epidemiology and Biostatistics, Faculty of Health Sciences, Universidad Cientifica del Sur, Lima, 15067, Peru;
6Grupo de Investigación Biomedicina, Faculty of Medicine, Fundación Universitaria Autónoma de las Américas-Institución Universitaria Visión de las Américas, Pereira, Colombia.
Article received 29 October 2024 and accepted 29 January 2025
Corresponding author
Alfonso J. Rodriguez-Morales
E-mail: arodriguezmo@cientifica.edu.pe
SummaRY
Introduction: The incidence of dengue and its complications increases globally, mainly in areas where it is endemic; however, little literature evaluates outcomes in kidney transplant recipients (KTR). The present analysis aimed to determine the incidence, signs and symptoms, and allograft dysfunction in dengue-infected KTR.
Methods: Systematic review of the literature following PRISMA 2020 indications with studies included until November 24, 2023.
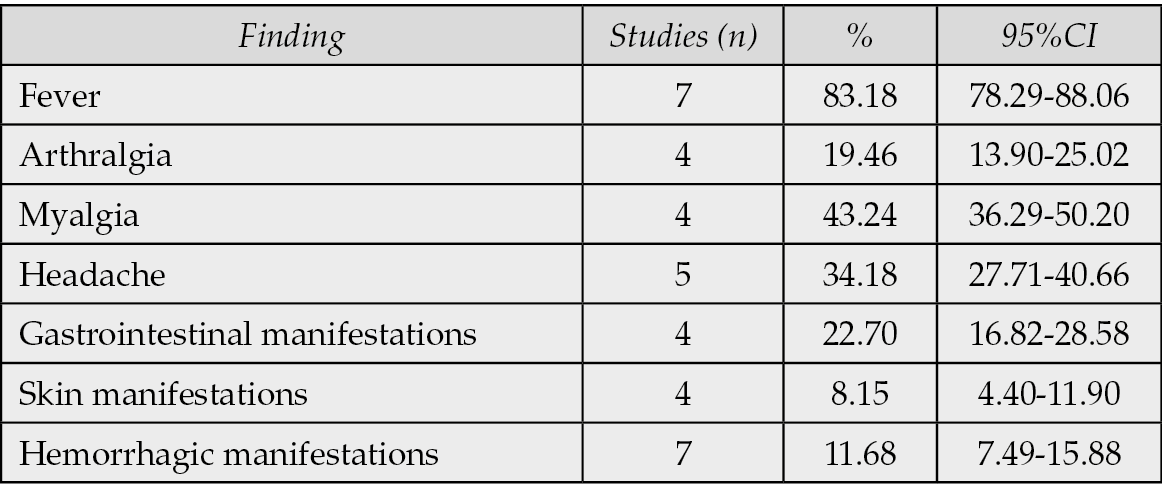
Results: Of 309 articles found, seven full-text studies were identified for analysis. 4337 KTRs with 214 dengue cases were evaluated. The incidence of dengue was 4.93%, varying between geographic regions. The average age was 41.50 years, and 61.21% were men. A mortality of 7.01% was reported. The symptoms were fever 83.18%, arthralgia 19.46%, myalgia 43.24% and headache 34.18%. The proportions of febrile dengue, with warning signs and severe dengue, were 63.55%, 23.83% and 11.68%, respectively. Transplant dysfunction and loss occurred in 63.08% and 4.67%, respectively.
Conclusions: Although the global distribution of dengue in KTR is unknown, there is a variable incidence between geographical areas and study times in which the KTR are evaluated. There is a high incidence of febrile symptomatology and transplant dysfunction consistent with global cohorts for non-KTR and KTR patients, respectively. Dysfunction is a prevalent event in KTRs with dengue infection, so correct screening should be done for donors and transplant candidates.
Keywords: Dengue, kidney, solid organ transplant, incidence.
INTRODUCTION
Dengue is a viral disease transmitted mainly by the Aedes aegypti and Aedes albopictus mosquitoes. It occurs worldwide in tropical and subtropical areas and is one of the most common vector-borne diseases [1]. Dengue virus (DENV) belongs to the Flaviviridae family and comprises four serotypes: DEN-1, DEN-2, DEN-3 and DEN-4. Infection with one of these serotypes does not confer long-lasting immunity. Infection with one serotype may be more severe if there has been a previous infection with another serotype [2]. In 2024, it has increased to more than 13 million reported cases in the Americas; however, many infected populations are asymptomatic [3, 4].
Currently, the disease is endemic in several countries located between Southeast Asia, Africa, the tropical Americas, the Eastern Mediterranean, the Western Pacific and even Africa. An analysis based on findings from the Global Burden of Diseases, Injuries and Risk Factors Study 2019 (GBD 2019) showed how globally, from 1990 to 2019, the incidence of dengue cases, deaths and disability-adjusted life years (DALYs) gradually increased [5]. There was the most rapid increase in incidence in East Asia in all regions (4.57 cases per 100,000 pop, 95%CI:4.31-4.82). Still, in Latin America, the highest mortality rates occurred (11.32 deaths per 100,000 pop, 95%CI:9.11-13.58) and age-standardized DALYs (4.13, 95%CI:2.98-5.29) [6].
Vectors transmit DENV; it has stages that range from mild fever to icterohemorrhagic fever, which, in many cases, is lethal [7]. However, most cases are asymptomatic; a meta-analysis of 131,953 cases showed a prevalence of asymptomatic DENV infections of 65.52% (95% CI: 38.73-92.32) during outbreaks and 30.78% (95% CI: 21.39-40.16) during non-outbreak periods [4]. Although the majority of cases are asymptomatic, mortality increases as DENV cases become more severe; a meta-analysis showed that the main factors associated with mortality in patients with dengue are severe hepatitis (Odds ratio [OR]=29.22 [95%CI:3.876-220.314)], dengue shock syndrome (OR=23.575, 95%CI:3.664-151.702), mental status alteration (OR=3.76, 95%CI:1.67-8.42), diabetes mellitus (OR=3.698, 95%CI:1.196–11.433) and higher heart rate (OR=1.039, 95%CI:1.011–1.067) [8].
Solid organ transplantation is a definitive and practical therapeutic option for patients with end-stage organ dysfunction such as liver, kidney, pancreas, heart and lung [9]. Renal transplantation (RT) is the preferred treatment for kidney failure, as it offers better quality of life and survival compared to dialysis and has also shown significantly lower mortalities. [10].
Despite the demonstrated benefits of transplantation, it is not always available in all geographic areas, it is not accessible to all types of patients, and some diseases can threaten the success of the transplanted patient, including diseases caused by arboviruses, especially in immunosuppressed hosts living in or travelling to endemic regions such as tropical or subtropical countries [11]. More significant immunosuppression may be associated with dengue [12]. A review in 2018 reported that according to series and case reports to that date in transplant patients, more than 95% of transplant recipients acquired dengue through vector transmission and that although mosquito bites are the frequent route, in the transplant recipient, there are other relevant sources of infection such as the graft itself and blood transfusions [11].
In 2017, the incidence and mortality from severe dengue were reported to be higher among transplanted patients compared with those without renal transplantation [13]. Additionally, there was a higher number of complications, overall mortality, and graft dysfunction. However, lack of data in this group of immunocompromised patients has not been identified due to a lack of screening and reporting, especially in low-income countries or countries with less comprehensive surveillance systems
The incidence of dengue and its complications is increasing in many regions where organ transplantation is frequent, mainly in hot or tropical regions where the disease is endemic [14-16]. Describing and understanding these phenomena is crucial because they can provide vital information on how this disease affects this sector of the immunocompromised population [16-20].
Recommendations for infection prevention in organ donors and recipients include identification of disabling organ compromise, treatment of infections, risk assessment, and implementation of preventive measures such as vaccination [19-21]. Standard screening tests usually detect herpesviruses, HIV, HBV, HCV, syphilis, and Toxoplasma gondii [21]. However, arboviruses are not usually screened, which increases risks in endemic regions [22]. Additionally, the risk of infection in transplant recipients depends on exposures and their “net immunosuppression status” [23]. Therefore, research is needed to support this high-risk group’s clinical decisions and public health policies [24]. This study aimed to conduct a systematic review describing the incidence of dengue in renal transplant patients and its outcomes in terms of severity, transplant involvement and mortality [1-54].
METHODS
Study type
A systematic or integrative review of the updated medical literature based on the PRISMA 2020 criteria was decided upon to carry out this thesis. This study aimed to estimate the incidence of dengue disease in patients with kidney transplants [25].
Databases
Free databases indexed via the Internet were included in the search for published literature. To search for medical literature, MeSH terms were used for PubMed and EMBASE and DeCS for the other two databases. Additionally, Google Scholar was used to complement the search results. The structure of the search formula is summarised in Table 1.
Table 1 - Search strategy and results by database.
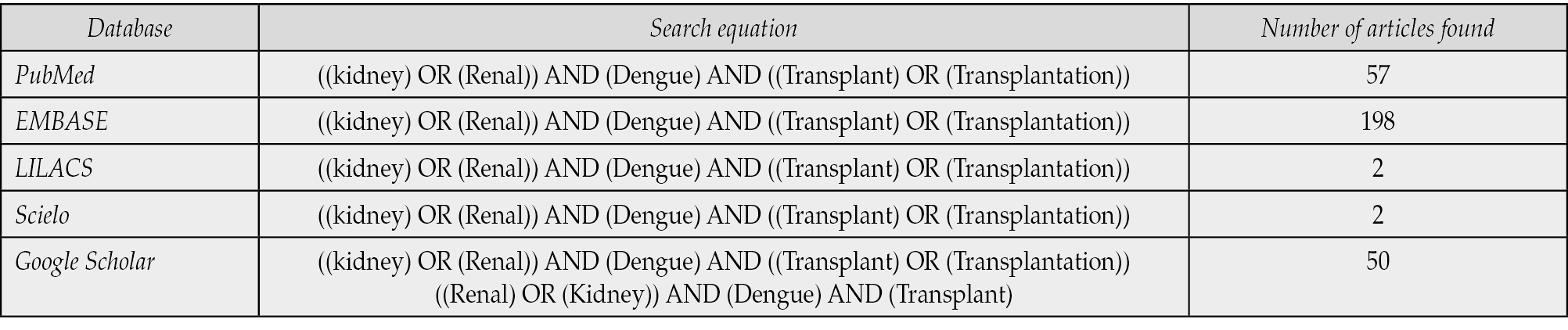
Search strategy
For this review, the search was carried out in the databases above with the combination of MesH terms: kidney, renal, dengue, transplant, and transplantation. The DeCS terms were also used: renal, kidney, dengue, and transplant. A secondary search was conducted by reviewing the reference lists of included articles to identify additional relevant studies. The search ended on November 24, 2023, without year-range restrictions, including all the historically available articles. The language of the articles was restricted to articles written in English or Spanish. In the search carried out in Google Scholar, the first fifty relevant articles were selected. The results of the database are summarised in Table 2.
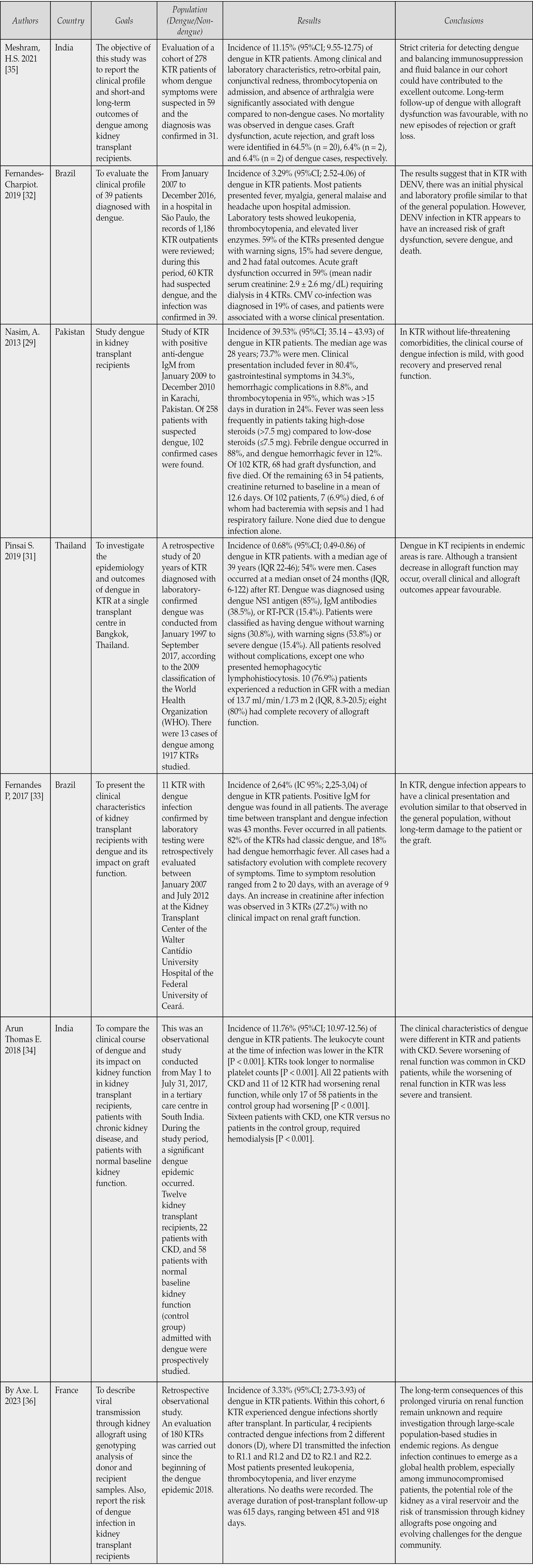
Table 2 - Summary of results. Characteristics of studies on the incidence of dengue infection in patients with kidney transplants.
Inclusion and exclusion criteria
We established our inclusion and exclusion criteria based on all case-control, cohort, and cross-sectional/ecological studies that reported the incidence of dengue in kidney transplant patients. Case reports and case series were excluded, as were clinical trial studies, letters to the editor, reviews, and abstracts presented at scientific meetings without sufficient data.
Data extraction
In an Excel template, the data were collected under the subheadings: names of the authors, type of study, city of origin, study period, Number of total participants (n) and were subsequently subdivided into those with and without dengue, signs, symptoms, laboratory data, dengue diagnostic technique, dengue severity, transplant dysfunction or loss, days of hospitalisation and death. We reviewed the titles and abstracts of the literature identified. All duplicate articles and literature not meeting the inclusion criteria were excluded. An expert evaluated abstracts considered potentially eligible for inclusion.
Assessment of risk of bias of individual studies
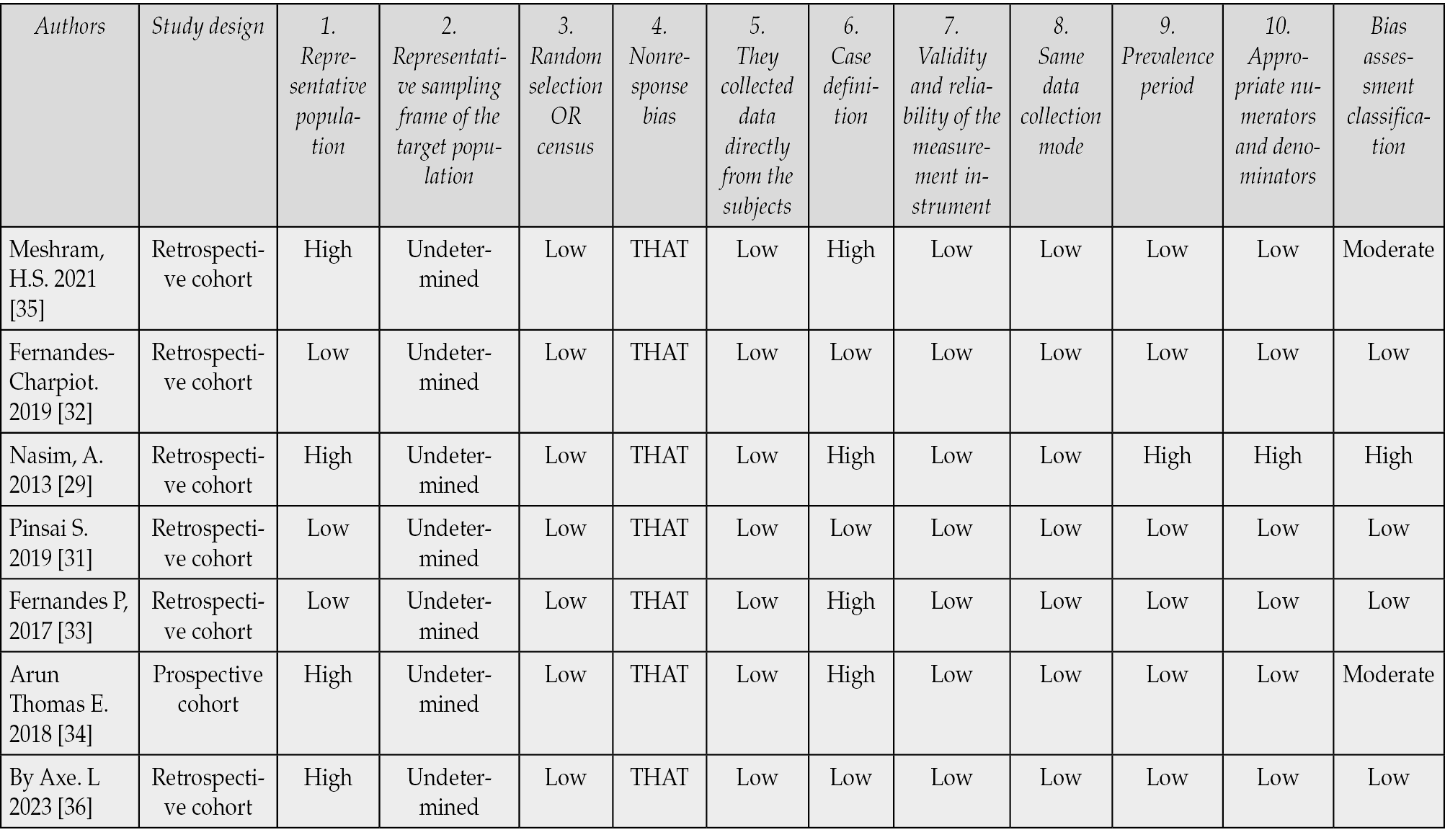
All studies were assessed for quality and bias in data analysis using an adapted version of the Risk of Bias Tool for Prevalence Studies developed by Hoy et al. [26]. This tool includes ten parameters that assess measurement, selection, and analysis bias. Each parameter is evaluated as high or low, and indeterminate was considered a high risk of bias. Bias was graded according to the number of high-risk bias parameters per study: low (≤2), medium (3–4), and high (≥5) [27]. This tool shows high inter-rater agreement when judging each item’s bias risk. In addition, the methodological quality criteria were used according to the manual strategies to rate the quality of the evidence and the strength of the recommendations using the GRADE approach [28].
Quality assessment using the GRADE tool found that all studies were of low quality as they were retrospective cohort studies carried out independently in different centres. Of the seven included studies, 4 (57.1%) were rated as having a low risk of bias, two as moderate (28.6%) and one as high (14.3%). High risk of bias ratings was most common for item 1 (representativeness), item 2 (target population), and item 6 (Case definition). The detailed results of the quality assessment of the seven studies are presented in Table 3. A funnel and Egger’s test assessed publication bias [29].
Table 3 - Assessment of risk of bias using an adapted version of the Risk of Bias Tool for Prevalence Studies.
Summary of the evidence
Data from all eligible articles were extracted using Microsoft Excel software tools version (2021 Microsoft 365, Microsoft Corporation®, USA). The incidence of dengue was calculated for each study using the number of cases reported in the sample as the numerator, divided by the total sample size as the denominator. All rates were calculated as the rate of dengue cases per 100 people, and the total sample is the sum of cases of kidney transplant patients with dengue and without dengue. To analyse the relevance or not of meta-analysis after carrying out the systematic review, a random effects model was used to add individual effect sizes and create a pooled incidence of DENV in TR when evaluating the heterogeneity between the studies using the statistical I2, heterogeneity between studies >75% was found, which is interpreted as high heterogeneity [30]. Given the above, it was not considered pertinent to perform a meta-analysis. All analyses were performed using the Stata statistical package, version 17.0.
RESULTS
The systematic literature search yielded 309 studies (Figure 1). After removing duplicates, 247 studies remained. Regarding selecting titles and abstracts to determine their relevance, 240 studies were excluded, giving seven full texts evaluated in the systematic review. Regarding potential bias publication, the shape of the funnel plot did not reveal apparent asymmetry except for one study with the highest incidence (Figure 2).
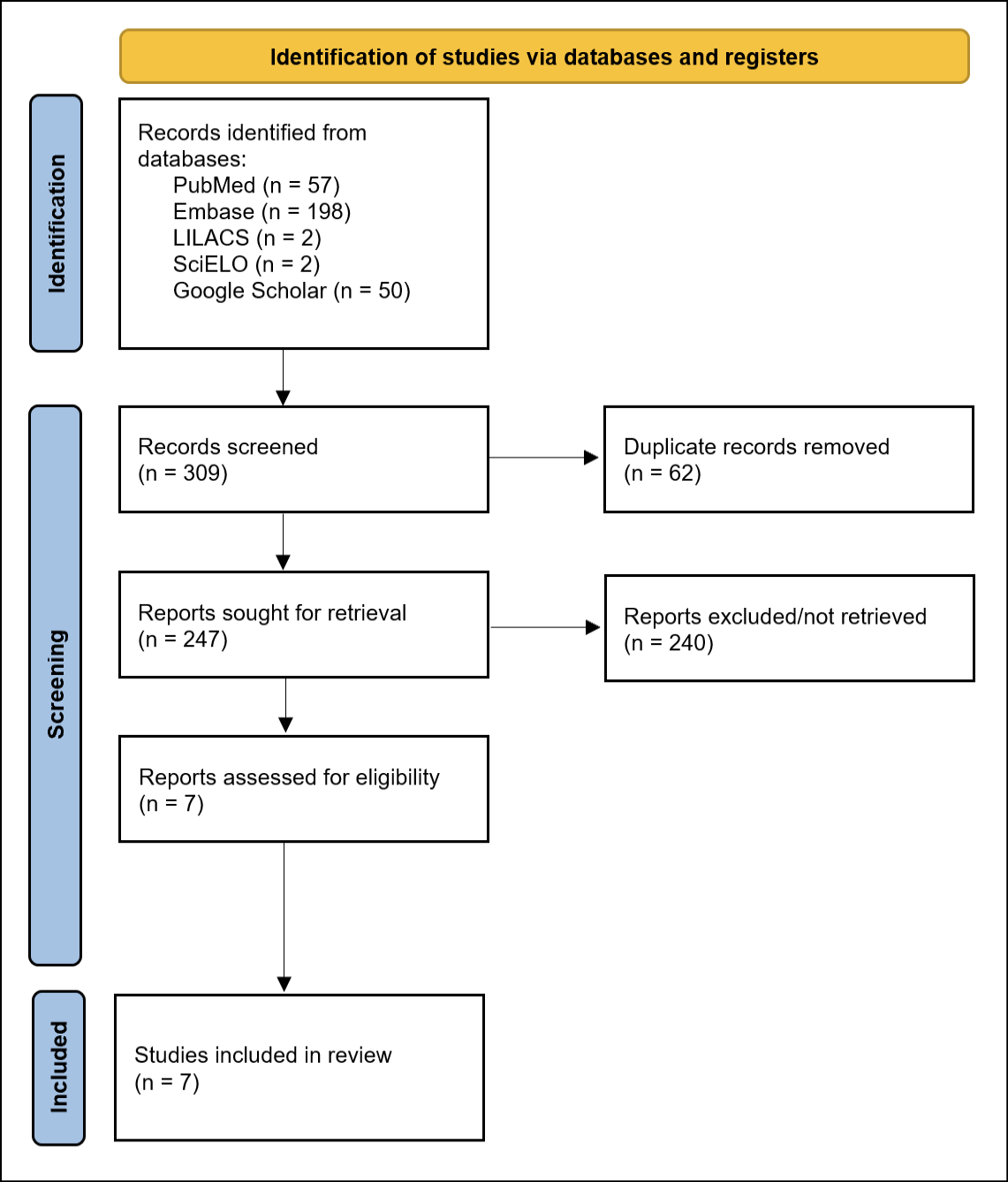
Figure 1 - Selection of studies according to PRISMA 2020 guidelines.
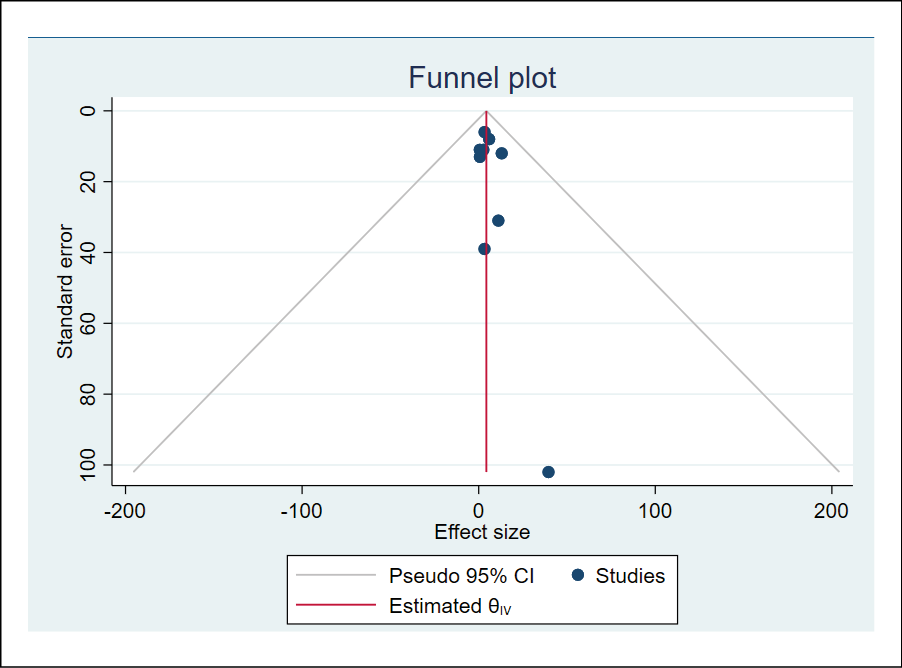
Figure 2 - Funnel plot and publication bias test by Egger test.
Most studies were conducted in Asia, India (n=2), Pakistan (n=1), and Thailand (n=1) followed by Brazil (n=2), and finally, a study was conducted in France. All included studies had designs such as retrospective cohort studies that included populations of both sexes and only an adult population after kidney transplantation. A total of 4337 KTR patients were evaluated across the studies, with 214 KTR cases with dengue infection. The incidence of dengue infection was 4.93% (95%CI:4.53-5.53) and this varied between 0.68% (95%CI:0.07-1.29) in the study by Pinsai S. and collaborators up to 39.53% (95%CI; 35.14-43.93) for the study by Nasim A. and collaborators which was carried out in a hyperendemic period of dengue in Pakistan [29,31]. A total of 15 deaths were reported throughout the studies for a proportion of 7.01% (95%CI:3.67%-10.34%) based on the 214 KTR patients with dengue analysed.
The average age of the patients throughout the studies was 41.50 years (95%CI; 40.20-42.80). The majority of patients in the included studies were men with an overall proportion of 61.21% (95%CI:54.85-67.58), however, for the Fernandes-Charpiot studies, Fernandes P and Thomas E [32-34]. The proportion of KTR women with dengue was 56.41% (95%CI; 41.11-71.72), 63.64% (95%CI; 35.59-91.69) and 91.67% (95%CI; 76.98-100.0) respectively. The results of NS1, IgM and PCR for identification of DENV infection were positive in 23.36% (95%CI:17.84-28.89), 78.50% (95%CI:73.14-83.87) and 11.68% (95%CI:7.49-15.88). An overview of the included studies on the incidence of dengue in kidney transplant patients is provided in Table 2. Table 4 summarises the main clinical findings of dengue among KTR.
Table 4 - Main clinical findings among KTR with dengue.
Dengue was classified by severity for all cohorts; incidences of febrile dengue, dengue with warning signs and severe dengue of 63.55% (95%CI:57.26-69.84), 23.83% were found (95%CI:18.27-29.40) and 11.68% (95%CI:7.49-15.88), respectively, the highest proportions of febrile dengue and severe dengue occurred in the cohort reported by Nasim A with 88.24% (95%CI:83.37-93.10) and 11.76% (95%CI:6.90-16.63) respectively; The remaining 1.4% (n=3) of patients were classified as dengue with an asymptomatic course despite their identification with IgM-DENV [36].
Transplant dysfunction was evaluated in all studies; this finding occurred in 63.08% (95%CI:56.78-69.39), and a proportion of allograft loss was found in 4.67% (95%CI:1.92%-7.43%). The highest proportions of transplant dysfunction were presented in the Pinsai S cohorts and Thomas E with incidence of dysfunction of 76.92% (95%CI:54.10-99.75) and 83.33% (95%CI:63.53-100.0) respectively [31,34].
The presentation of thrombocytopenia was evaluated in all studies; however, for Thomas E, only the mean values of the platelet count are reported in general, thrombocytopenia had a proportion of 87.13% (95%CI:82.62%-91.64%), with the highest incidences being those reported in Meshram’s studies [34]. H.S (35) y Nasim A (29) with proportions of 93.55% (95%CI:85.40-100.0) and 95.10% (95%CI:91.76-98.43) respectively. Leukopenia was reported in 5 studies, finding a general proportion of 65.82% (95%CI:59.34%-72.29%) with an average value of the leukocyte count of 3143.8 (95%CI:2981.0-3306.6), the highest incidence of leukopenia was reported by Nasim A with 70.59% (95%CI:63.71-77.46) [29,31-33,35].
Mean creatinine values were reported in 4 studies with a mean baseline creatinine of 1.43 mg/dL SD 0.22 (95%CI:1.40-1.46) and creatinine during the nadir of infection of 2.24 mg/dL SD 0.48 (95%CI:2.17-2.31) [29,31-33]. Elevation of liver enzymes was reported in 5 studies with a proportion of 45.0% (95%CI:35.37-54.63) [31-33,35,36]. Only three studies reported coinfection with CMV in a total of 28.49% (95%CI:22.09-34.89) of the KTRs, with the highest proportion reported by Nasim A of 37.25% (95%CI:29.09-34.89) [29,32,35]. 96-44.55) of the KTRs included with DENV in their cohort. Throughout the reports, only 2.34% (95%CI:0.36-4.31) of KTRs with DENV infection required dialysis.
The study with the highest cut-off within the present analysis was conducted by Pinsai et al. [31]; this study describes that dengue in RT recipients in endemic areas is rare. Although a transient decrease in allograft function may occur, overall clinical and allograft outcomes appear favorable. However, we know that in other retrospective trials, an increase in hospital stay and use of medical supplies for diagnosis and treatment can be identified in this group of patients with unique characteristics [33,35].
On the other hand, when dividing by graphs, it was identified that in areas such as Southeast Asia, where there is the highest incidence of dengue, patients with kidney transplants are mainly associated with the presence of studies carried out in endemic peaks [29]. Alerts are raised at an epidemiological level about these data identified in different areas of the world, but mainly Asia, which is a potential source of study and characterization of risk factors for the spread of dengue in this group of patients.
DISCUSSION
A total of 4337 patients were evaluated throughout the studies, with 214 dengue cases. The incidence of dengue infection was 4.93% (95%CI:4.53-5.53), which varied between 0.68% and 39.53% throughout the KTRs.
The incidence of symptomatic dengue was 4.93% in transplant patients, showing a higher incidence than in the general population. For example, in the Americas, the average incidence in 2024 was 1.29% (1,289.31 cases per 100,000 inhabitants), and even higher than in the subregion with the highest incidence in the Americas, the Southern Cone, where it was 3.78% (3,779.5 cases per 100,000 inhabitants). When grouping data according to severity, the incidence of severe dengue was 11.68%, which was also higher than in the general population. Finally, the average incidence of severe dengue in 2024 was 0.17%, compared to the country in the Americas with the highest severe dengue incidence. Compared to Puerto Rico, reporting 5.27% in 2024, such incidence among the KTR population remains considerably higher (https://www3.paho.org/data/index.php/en/mnu-topics/indicadores-dengue-en/dengue-regional-en/317-reg-dengue-lethality-en.html).
This higher incidence could partly be explained by geographic variations and the fact that transplant patients receive more comprehensive care and undergo more active infection screening than the general population. This explanation might also apply to transplant dysfunction, which in our study occurred in 63.08% (95%CI: 56.78-69.39), with a proportion of allograft loss found to be 4.67% (95%CI: 1.92%-7.43%).
On the other hand, the data presented show an overall mortality (case fatality rate, CFR) of 7.01% (95%CI: 3.67%-10.34%). The CFR in the Americas for dengue in the general population, in 2024, was 0.063%. The CFR among KTR patients is higher than the highest CFR of the Americas, in the Latin Caribbean, which is just 0.112% among the general population.
In dengue infection, a recent meta-analysis found a mean mortality rate of 5.13% (95%CI:0.01%-38.68%) with factors such as dengue syndrome, dengue shock (OR=23.575, 95%CI:3.664-151.702), altered mental status (OR=3.76, 95%CI:1.67-8.42) and diabetes mellitus (OR=3.698, 95%CI:1.196-11.433), factors associated with mortality [38]. A study with patients with TR from 1980 to 2018 that covered 23,210 KTR recorded 4,765 (20.53%) deaths with functional graft were reported [39]. The data presented throughout the literature show lower mortality rates than those presented in this review in patients with non-KTR dengue and higher in KTR patients, which could explain the midpoint of the proportion reported by our analysis, which includes KTR patients infected by dengue; it is worth highlighting that throughout the studies gathered in this analysis, the deaths in KTR patients infected by DENV in most cases were accompanied by another complication or coinfection that caused death; therefore, the low mortality compared to cohorts of KTR patients may not only be associated with underestimation of cases but also with the lack of timely identification in the donor and the DENV patient.
The average age of the patients throughout the studies was 41.50 years (95%CI:40.20-42.80), with 61.21% being men (95%CI:54.85-67.58) of the cases. By focusing on the TR field, the data compared to global studies reveal that the majority of transplants are performed in adult men under the age of 60, cohort studies in 2016 with 1,946 KTR with 95.5% <60 years and 67.3% and a study in 2023 with 45,912 KTR with a mean (SD) age of 54.3 (13.2) and 60.9% men corroborate the data found in these cohorts [40, 41]. On the other hand, the age range and gender of infection in dengue place the infection in young female patients. A multicenter prospective cohort study in Brazil found that 49.1% of dengue cases are between 18 and 49 years old, and 60.4% are women [42]. The data found by this cohort urges the search for screening and prevention measures for dengue infection in KTR and donors at young ages, given that they are the most seroprevalent groups.
The clinical presentation of dengue among KTR is similar to those with infection among the general population, with fever, arthralgia, myalgia, and headache, among others. In the meta-analysis published in 2017, the KTR patients with dengue infection evaluated found proportions of fever of 91.3%, myalgia at 95.5%, arthralgia at 25% in addition to proportions of new hemorrhagic complications at 34.8%, headache at 91.3%, diarrhoea 15.3%, pleural effusion 84.6% and ascites 38.5% [13]. The data presented by the current analysis demonstrate a high prevalence of febrile events, arthralgia, and consistent headache in patients with TR and those without TR, indicating that the diagnostic suspicion based on clinical symptoms could be the same in patients with and without TR.
On the other hand, the proportions of febrile dengue, dengue with warning signs, and severe dengue were 63.55% (95%CI:57.26-69.84), 23.83% (95%CI:18.27-29 .40) and 11.68% (95%CI:7.49-15.88) respectively. Retrospective cohort studies in non-KTR patients found proportions of non-severe dengue between 65% and 74.3% and severe dengue between 24.7% and 35% (43,44). These results reflect similar rates for non-severe dengue but lower rates for severe dengue in our study. These data could indicate a lower pathogenicity mediated by a deficient immune response from immunosuppressive medications. A recent review that addresses the issue of sick viral ages in immunocompromised patients postulates that immunocompromised patients receiving biologic medications are not at increased risk of viral disease severity and suggests that reduced immune reactivity may contribute to dampening the pathogenic mechanisms induced by cytokine storm in viral and arboviral diseases [18]. However, this hypothesis arises from the efficacy of immunosuppressive treatment proven in several randomised controlled trials to benefit survival in non-immunocompromised patients with SARS-CoV-2 infection. More studies are needed to define the disease’s behaviour in these groups, including dengue in immunocompromised patients and dengue in KTR patients.
Immunosuppression in transplanted patients with dengue can worsen the infection’s course, increasing the risk of severe disease due to impaired immune response. Dengue’s thrombocytopenia and vascular permeability can compound transplant-related complications. A clinical pathway includes closely monitoring platelet levels, liver function, and signs of organ rejection. Temporarily reducing or adjusting immunosuppressive drugs, particularly antimetabolites, may be considered under expert guidance to balance infection control and rejection prevention. Supportive care, hydration, and timely management of complications are essential. Collaboration between transplant specialists and infectious disease experts is critical to optimise outcomes while minimising risks associated with dengue and graft rejection [53].
Transplant dysfunction occurred in 63.08% (95%CI:56.78-69.39), and a proportion of allograft loss was found in 4.67% (95%CI:1.92%-7.43%) throughout the KTR analyses with DENV infection. As previously presented, the role of arboviral infections in KTR is not fully understood; however, viral infections have a clinical impact on the outcomes of KTR patients. A study published in 2019 found that CMV and HCV viral infections are associated with complications as well as graft failure in kidney transplant recipients [45].
Viral infections have previously been found to be associated with kidney transplant complications and graft rejection. It is known that the incidence of CMV infection is high among KTRs and is considered responsible for the deterioration of graft function. kidney and graft failure, mainly responsible for the high rates of post-kidney transplant morbidity and mortality (46); it is also notable that in the analysis of 3 of the studies, an incidence of up to 28.49% (95%CI:22.09-34.89) in KTR patients infected by DENV was reported. The results obtained in different studies throughout the literature could help guide the view on viral diseases and their role in the outcomes of patients with solid organ transplants. In the case of dengue, we can observe an essential impact on the loss of the graft function reported in our study. However, complete graft loss had a low incidence.
The overall proportions of thrombocytopenia, leukopenia and liver enzyme alteration were 87.13%, 65.82%, and 45.0%, respectively, similar to dengue among the general population. In a study, significant laboratory alterations were found, including thrombocytopenia (87.0%), leukopenia (51.7%) and abnormalities in liver function tests (69.0%) were identified as the clinical alterations most commonly presented by KTRs with dengue [13]. A retrospective cohort study carried out in patients with non-KTR dengue in 2016 found that not only is thrombocytopenia common in patients with dengue, but it has a direct correlation with the complications and duration of hospitalisation (p<0.001) [47]. On the other hand, a retrospective study determined statistically that the higher the percentage of lymphocytes, the faster the recovery from dengue and the shorter the hospital stay [48]. The data presented by the previous review and the present one tend to have similar proportions in terms of laboratory values throughout the included studies; however, the relevant point of these data is complemented by the findings throughout the literature where it is observed how the platelet and lymphocyte count could predict results on hospitalisation and survival of patients infected by DENV, even so, prospective cohort studies of a more significant number of patients and with a longer follow-up which include KTR patients are necessary to determine the effect of these cell counts on this population.
Dengue is presented as a risk factor for the deterioration of kidney function in healthy patients; however, its effect on the kidney function of immunocompromised patients is unknown. A meta-analysis published in 2023 found that the pooled incidence of ARI in patients with dengue was 8.0% (95%CI:6%-11%), with a high heterogeneity between the studies. This study revealed a high incidence of ARF in dengue patients, underscoring the need for regular kidney examinations to detect ARF early and reduce the risk of hospitalisation [49]. For our review, the average creatinine values were 1.43 mg/dL at baseline, SD 0.22 (95%CI:1.40-1.46) and creatinine during the nadir of infection was 2.24 mg/dL, SD 0.48 (95%CI:2.17-2.31). Data from cohorts included in this analysis reveal an essential change in renal function in DENV-infected KTR patients, which is directly related to the data above on transplant dysfunction and also has an impact on survival and survival rates. hospitalisation in KTR patients. These two results force us to reevaluate the need for timely screening for dengue in donors, mainly in endemic areas, and an active search for infection when symptoms are suspected.
The main strength of the present study is the ability to select the most up-to-date literature and studies of better methodological quality compared to previous reviews, as well as a more significant number of patients undergoing kidney transplantation with a discrete incidence of KTR patients with dengue infection in areas endemic. The weaknesses of the present study are mainly those associated with its nature, such as the moderate quality studies included for the analysis given its observational nature, as well as the inability to make specific risk estimates on relevant clinical outcomes as it is not possible. Given the high heterogeneity among the included studies, the comparison through a meta-analysis with another group of studies was not possible.
Finally, given the availability of Dengue vaccination, this offers significant benefits for patients on transplantation waiting lists and post-transplantation by reducing dengue infection risk and severity, especially in endemic areas. Pre-transplant patients benefit from vaccination to prevent delays caused by infections, but vaccination should occur before transplantation for optimal immune response. Post-transplant patients on immunosuppressants face reduced vaccine efficacy and heightened risks if seronegative. Serostatus testing is crucial, as vaccines like Dengvaxia® (Sanofi) are recommended only for seropositive individuals; or new vaccines, such as Qdenga® (Takeda), which can be used regardless of serostatus. Vaccination should align with broader prevention strategies, including vector control and patient education. Research is needed to ensure vaccine safety and efficacy in immunocompromised populations and to develop vaccines suitable for both seropositive and seronegative patients. Careful assessment and follow-up are essential [54].
CONCLUSIONS
Tropical diseases in renal transplant patients pose a clinical challenge [50]. The incidence of dengue varies according to geographic area, time of year, and patient-specific factors [51]. This analysis documented similar rates of non-severe dengue but lower rates of severe dengue in KTR patients than in non-KTR patients and further demonstrated a high incidence of febrile episodes, arthralgias, and headaches in both KTR and non-KTR patients, indicating that the diagnostic suspicion based on clinical findings may be the same in KTR and non-KTR patients. On the other hand, renal dysfunction is a prevalent event in KTR with DENV infection. All this argues that screening for DENV infection would be justified in donors and transplant candidates in endemic regions to avoid possible complications or even graft loss.
Conflict of interest
AJRM has been declared a speaker/consultant in the last decade for the following industries involved in dengue and arbovirus vaccines: Sanofi Pasteur, Abbott, Takeda, MSD, Moderna, and Valneva.
Funding
None
Acknowledgements
This study was partly presented at the XIV National Meeting of Research and Innovation in Infectious Diseases of the Colombian Association of Infectious Diseases (ACIN) and IV Latin American Meeting of Research in Infectious Diseases, Medellin, Colombia, September 26-28, 2024. Dr Rodriguez-Morales would like to dedicate this publication to the memory of Prof. Olinda Delgado, PhD (1930–2024), an expert in tropical and parasitic diseases such as leishmaniasis and toxocariasis, from Venezuela, his major mentor and excellent human being, who passed away in Caracas, December 2024, R.I.P. This article has been registered in the Research Proposal Registration of the Coordination of Scientific Integrity and Surveillance of Universidad Cientifica del Sur, Lima, Peru, under the number PI-50-2025-0067.
REFERENCES
[1] Rodriguez-Morales AJ, Montenegro-Idrogo JJ, Celis-Salinas JC, et al. Unraveling the unparalleled 2024 epidemic of Dengue in the Americas. Rev Chilena Infectol 2024; 41(3): 421-428. doi 10.4067/s0716-10182024000300133.
[2] Kok BH, Lim HT, Lim CP, Lai NS, Leow CY, Leow CH. Dengue virus infection - a review of pathogenesis, vaccines, diagnosis and therapy. Virus Res. 2023; 324: 199018.
[3] WHO. Dengue and severe dengue. 2019. www.who.int, accessed January 10, 2025.
[4] Asish PR, Dasgupta S, Rachel G, Bagepally BS, Girish Kumar CP. Global prevalence of asymptomatic dengue infections-a systematic review and meta-analysis. Int J Infect Dis. 2023; 134: 292-298.
[5] Yang X, Quam MBM, Zhang T, Sang S. Global burden for dengue and the evolving pattern in the past 30 years. J Travel Med. 2021; 28(8): taab146.
[6] Tian N, Zheng JX, Guo ZY, et al. Dengue Incidence Trends and Its Burden in Major Endemic Regions from 1990 to 2019. Trop Med Infect Dis. 2022; 7(8): 180.
[7] Wang WH, Urbina AN, Chang MR, et al. Dengue hemorrhagic fever – A systemic literature review of current perspectives on pathogenesis, prevention and control. J Microbiol Immunol Infect. 2020; 53 (6): 963-978.
[8] Chagas GCL, Rangel AR, Noronha LM, et al. Risk factors for mortality in patients with dengue, A systematic review and meta-analysis. Trop Med Int Health. 2022; 27(8): 656-668.
[9] Black CK, Termanini KM, Aguirre O, Hawksworth JS, Sosin M. Solid organ transplantation in the 21st century. Ann Transl Med. 2018; 6(20): 409-409.
[10] Tonelli M, Wiebe N, Knoll G, et al. Systematic Review: Kidney Transplantation Compared With Dialysis in Clinically Relevant Outcomes. Am J Transplant. 2011; 11(10): 2093-2109.
[11] Darrigo LG, St. Anna Carvalho AM, Machado CM. Chikungunya, Dengue, and Zika in Immunocompromised Hosts. Curr Infect This Rep. 2018; 20(4): 5.
[12] Tsai CL, Sun DS, Su MT, et al. Suppressed humoral immunity is associated with dengue nonstructural protein NS1-elicited anti-death receptor antibody fractions in mice. Sci Rep. 2020; 10(1): 6294.
[13] Weerakkody RM, Patrick JA, Sheriff MHR. Dengue fever in renal transplant patients: a systematic review of literature. BMC Nephrol. 2017; 18(1): 15.
[14] Mulligan K, Dixon J, Joanna Sinn CL, Elliott SJ. Is dengue a disease of poverty? A systematic review. Pathog Glob Health. 2015; 109(1): 10-18.
[15] Codeco CT, Oliveira SS, Ferreira DAC, et al. Fast expansion of dengue in Brazil. The Lancet Regional Health-Americas. 2022 Aug; 12: 100274.
[16] Santos RP dos, Carvalho AR da S, Peres LAB. Kidney transplantation epidemiology in Brazil. Nephrology. 2019; 39(4): 402-410.
[17] Rosso F, Sanz AM, Parra-Lara LG, Moncada PA, Vélez JD, Caicedo LA. Dengue Virus Infection in Solid Organ Transplant Recipients: A Case Series and Literature Review. Am J Trop Med Hyg. 2019; 101(6): 1226-1231.
[18] Agrati C, Bartolini B, Bordoni V, et al. Emerging viral infections in immunocompromised patients: A great challenge to better define the role of immune response. Front Immunol. 2023; 14: 1147871.
[19] Alberú J, Urrea EM. Immunosuppression for kidney transplant recipients: current strategies. Rev Invest Clin. 2005; 57(2): 213-224.
[20] Fischer SA, Lu K. Screening of Donor and Recipient in Solid Organ Transplantation. Am J Transplant. 2013; 13 Suppl. 4 (Suppl. 4): 9-21.
[21] Sawinski D, Blumberg EA. Infection in Renal Transplant Recipients. In: Chronic Kidney Disease, Dialysis, and Transplantation. Elsevier; 2019; 621-638.e6.
[22] Moura-Neto JA, Braga Silva CA, Moura AF, Rocco Suassuna JH. Emergent Arboviruses and Renal Transplantation: A Global Challenge. Kidney Int Rep. 2019; 4(5): 647-655.
[23] Fishman JA, Costa SF, Alexander BD. Infection in Kidney Transplant Recipients. In: Kidney Transplantation-Principles and Practice. Elsevier. 2019; 517-538.
[24] Wang Y, DelRocco N, Lin L. Comparisons of various estimates of the I2 statistic for quantifying between-study heterogeneity in meta-analysis. Stat Methods Med Res. 2024; 33(5): 745-764. doi: 10.1177/09622802241231496.
[25] Page MJ, McKenzie JE, Bossuyt PM, et al. PRISMA 2020 statement: an updated guide for the publication of systematic reviews. Rev Esp Cardiol. 2021; 74(9): 790-799.
[26] Hoy D, Brooks P, Woolf A, et al. Assessing risk of bias in prevalence studies: modification of an existing tool and evidence of interrater agreement. J Clin Epidemiol. 2012; 65(9): 934-939.
[27] Olivera MJ, Fory JA, Porras JF, Buitrago G. Prevalence of Chagas disease in Colombia: A systematic review and meta-analysis. PLoS One. 2019; 14(1): e0210156.
[28] Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008; 336(7650); 924-926.
[29] Nasim A, Anis S, Baqi S, Akhtar SF, Baig-Ansari N. Clinical presentation and outcome of dengue viral infection in live-related renal transplant recipients in Karachi, Pakistan. Transpl Infect Dis. 2013; 15(5): 516-525.
[30] Migliavaca CB, Stein C, Colpani V, et al. Meta-analysis of prevalence I2 statistic and how to deal with heterogeneity. Res Synth Methods. 2022; 13(3): 363-367.
[31] Pinsai S, Kiertiburanakul S, Watcharananan SP, Kantachuvessiri S, Boongird S, Bruminhent J. Epidemiology and outcomes of dengue in kidney transplant recipients: A 20-year retrospective analysis and comparative literature review. Clin Transplant. 2019; 33(1): e13458.
[32] Fernandes-Charpiot IMM, Estofolete CF, Caldas HC, et al. Clinical and laboratorial profiles of dengue virus infection in kidney transplant recipients: Report of a single center. PLoS One. 2019; 14(10): e0219117.
[33] Fernandes PFCBC, Siqueira RA, Girão ES, et al. Dengue in renal transplant recipients: Clinical course and impact on renal function. Transplant World J. 2017; 7(1): 57.
[34] Thomas ETA, George J, Sruthi D, Vineetha NS, Gracious N. Clinical course of dengue fever and its impact on renal function in renal transplant recipients and patients with chronic kidney disease. Nephrology. 2019; 24(5): 564-568.
[35] Meshram HS, Kute V, Patel H, Banerjee S, Chauhan S, Desai S. Successful management of dengue in renal transplant recipients: A retrospective cohort from a single center. Clin Transplant. 2021; 35(7): e14332.
[36] Di Ascia L, Jaffar-Bandjee MC, Cresta MP, et al. Dengue Virus in Kidney Allograft: Implications for Donor Screening and Viral Reservoir. Kidney Int Rep. 2024; 9(1): 186-190.
[37] Murhekar M V, Kamaraj P, Kumar MS, et al. Burden of dengue infection in India, 2017: a cross-sectional population based serosurvey. Lancet Glob Health. 2019; 7(8): e1065-e1073.
[38] Chagas GCL, Rangel AR, Noronha LM, et al. Risk factors for mortality in patients with dengue: A systematic review and meta-analysis. Trop Med Int Health. 2022; 27(8): 656-668.
[39] Ying T, Shi B, Kelly PJ, Pilmore H, Clayton PA, Chadban SJ. Death after Kidney Transplantation: An Analysis by Era and Time Post-Transplant. J Am Soc Nephrol. 2020; 31(12): 2887-2899.
[40] Ozkul F. Effect of Age on The Outcome of Renal Transplantation: A Single-Center Experience. Pak J Med Sci. 2016; 32(4): 827-830.
[41] Ji M, Vinson AJ, Chang SH, et al. Patterns in Use and Transplant Outcomes Among Adult Recipients of Kidneys From Deceased Donors With COVID-19. JAMA Netw Open. 2023; 6(5): e2315908.
[42] de Aguiar DF, de Barros ENC, Ribeiro GS, et al. A prospective, multicentre, cohort study to assess the incidence of dengue illness in households from selected communities in Brazil (2014-2018). Int J Infect Dis. 2021; 108: 443-453.
[43] Sami CA, Tasnim R, Hassan SS, Khan AH, Yasmin R, Monir-uz-Zaman M, et al. Clinical profile and early severity predictors of dengue fever: Current trends for the deadliest dengue infection in Bangladesh in 2022. IJID Regions. 2023; 9: 42-48.
[44] Agrawal VK, Prusty BSK, Reddy CS, Mohan Reddy GK, Agrawal RK, Sekher Srinivasarao Bandaru VC. Clinical profile and predictors of Severe Dengue disease: A study from South India. Caspian J Intern Med. 2018; 9(4): 334-340.
[45] Syu SH, Lin YW, Lin KH, Lee LM, Hsiao CH, Wen YC. Risk factors for complications and graft failure in kidney transplant patients with sepsis. Bosn J Basic Med Sci. 2018; 19(3): 304-311.
[46] Al Atbee MYN, Tuama HS. Cytomegalovirus infection after renal transplantation. J Med Life. 2022; 15(1): 71-77.
[47] Jayanthi H, Tulasi S. Correlation study between platelet count, leukocyte count, nonhemorrhagic complications, and duration of hospital stay in dengue fever with thrombocytopenia. J Family Med Prim Care. 2016; 5(1): 120.
[48] Ananda Rao A, U RR, Gosavi S, Menon S. Dengue Fever: Prognostic Insights From a Complete Blood Count. Cureus. 2020; 12(11): e11594.
[49] Bushi G, Shabil M, Padhi BK, et al. Prevalence of acute kidney injury among dengue cases: a systematic review and meta-analysis. Trans R Soc Trop Med Hyg. 2023; 118(1): 1-11. doi: 10.1093/trstmh/trad067.
[50] Franco-Paredes C, Jacob JT, Hidron A, Rodriguez-Morales AJ, Kuhar D, Caliendo AM. Transplantation and tropical infectious diseases. Int J Infect Dis. 2010; 14(3): e189-e196. doi: 10.1016/j.ijid.2009.04.021.
[51] Rodríguez-Morales AJ, López-Medina E, Arboleda I, et al. The epidemiological impact of dengue in Colombia: a systematic review. Am J Trop Med Hyg. 2024; 112(1): 182-188. doi 10.4269/ajtmh.23-0907
[52] Rodríguez-Morales AJ, López-Medina E, Arboleda I, et al. Cost of dengue in Colombia: A systematic review. PLoS Negl Trop Dis. 2024; 18(12): e0012718. doi: 10.1371/journal.pntd.0012718.
[53] Sohail A, Zhong S, Nguyen PY, McGuinness SL, Leder K. Dengue fever in immunocompromised patients: A systematic review and meta-analysis. Int J Infect Dis. 2024; 149: 107272. doi: 10.1016/j.ijid.2024.107272.
[54] Sirivichayakul C, Biswal S, Saez-Llorens X, et al. Efficacy and Safety of a Tetravalent Dengue Vaccine (TAK-003) in Children With Prior Japanese Encephalitis or Yellow Fever Vaccination. J Infect Dis. 2024; 230(6): e1214-e1225. doi: 10.1093/infdis/jiae222.