Le Infezioni in Medicina, n. 1, 130-138, 2025
doi: 10.53854/liim-3301-13
CASE REPORTS
Syphilitic pneumonia: case report and systematic review
Giuseppe Pipitone1, Michelle Abbott1, Andrea Gizzi1, Calogero Buscemi1, Federica Guida Marascia1, Claudia Imburgia1, Giacomo Ciusa1, Alba La Sala2, Giuseppe Giorgio Mancuso3, Domenico Messana4, Antonio Cascio5, Chiara Iaria1.
1 Infectious Disease Unit, ARNAS Civico-Di Cristina, Palermo, Italy;
2 Bronchial Endoscopy Unit, ARNAS Civico-Di Cristina, Palermo, Italy;
3 Pathology, Buccheri La Ferla Hospital, Palermo, Italy;
4 Radiology, ARNAS Civico-Di Cristina, Palermo, Italy;
5 Infectious Disease Unit, University Hospital P. Giaccone, Palermo, Italy.
Article received 28 October 2024 and accepted 21 January 2025
Corresponding author
Giuseppe Pipitone
E-mail: pep2pe@gmail.com
SummaRY
Syphilitic pneumonia is a rare secondary form of Treponema pallidum infection. In this article, we present a case of syphilitic pneumonia in a patient living with Human Immunodeficiency Virus (HIV) with good immune-virological status. We also performed a systematic review of literature and we found 43 cases of syphilitic pneumonia described since 1886. We added our case report and performed a statistical analysis. Our analysis showed that 40/44 (91%) were males, with a median age of 46 years old (IQR 37-56), 9/28 (32%) were people living with HIV (data not available for 16/44 patients), 17/27 (63%) had syphilitic-related hepatitis during the clinical presentation (data not available for 17/44 patients), and 28/42 (66.6%) of patients had maculopapular rash compatible with secondary forms (data not available for 2/42 patients).
Furthermore, 74.4% of patients had nodular lesions on chest X-ray or pulmonary Computed Tomography scan. Given the high rate of nodular pneumonia among patients, clinicians should consider it as a common presentation in syphilitic pneumonia
Keywords: syphilis, pulmonary syphilis, syphilitic pneumonia, nodular lesions, atypical pneumonia.
INTRODUCTION
Syphilis is a sexually transmitted infectious disease (STD) caused by the spirochete Treponema pallidum subp. pallidum (T. pallidum). Recognized as a significant public health challenge for centuries, over the last few years it was observed an increase in syphilitic cases, particularly in certain populations and geographical areas, making it a persistent concern for healthcare providers and public health officials. During the last decades, emerging trends of syphilis incidence has been noticed worldwide, especially among Male who have Sex with Man (MSM), People Who Injected Drugs (PWID) and People Living with HIV (PLWH). Amongst these populations, clinical presentation may differ, sometimes due to immune alteration (i.e. HIV) and therefore diagnosis can be difficult [1-3]. So, syphilitic infection has become a public health challenge, as well as Monkeypox outbreaks, which affects similar at-risk population and both diseases may have similar cutaneous presentations [4, 5].
Syphilis is well-known as “the great imitator”, given the wide range of clinical manifestations, typically ranging from the chancre of the primary form to the mucocutaneous lesions of the secondary forms, and the Central Nervous System involvement of the tertiary forms (sometimes may be a manifestation of early neurosyphilis). Due to the multi-organ involvement, signs and symptoms of secondary and tertiary forms are more complex and/or blurred, and often under-recognized. For example, rare secondary forms manifestations may be hepatitis or pneumonia. Although it is considered a rare presentation, pneumonia is not a novelty and the first case report in literature was published in 1886 [6, 7]. This condition, often unrecognized, let us understand the importance of considering syphilis in the differential diagnosis of pneumonia, especially in patients with risk factors for sexually transmitted diseases. Patients with syphilitic pneumonia have classical respiratory symptoms such as cough, fever, dyspnea and chest pain, mimicking other infectious and non-infectious lung diseases [6, 7]. Defined as a secondary syphilitic form, the gold standard therapy remains i.m. benzylpenicillin 2.4 MU, with a favorable prognosis after treatment. However, delayed diagnosis and treatment may lead to complications, underscoring the importance of early recognition and intervention. In this article we present a case of syphilitic pneumonia in an HIV-infected patient and a review of the literature on similar syphilitic presentations.
CASE REPORT
A 31-year-old man who have sex with man (MSM), living with HIV and with mild dyslipidemia went to our Emergency Room (ER). Two months earlier he performed a routinary blood test in our outpatients clinic, which showed a good immune-virological status: HIV-RNA not detected, CD4+ count 597/uL (30%), CD4+/CD8+ ratio 0.7, RPR and TPPA serology were negative. He presented with fever, asthenia, vomiting, and abdominal pain lasting for a few days, so he was admitted to our Infectious Disease Unit, ARNAS Civico, Palermo (Italy). The patient was alerted and oriented, he had arterial pressure of 100/60 mmHg, SpO2 95% in room air, a heart rate of 88 bpm, and a body temperature of 37.2 C. Physical examination showed a non-pruritic papular-erythematous skin rash on the trunk, back, limbs, and palms of the hands with mild sweating; at abdominal examination, the patient had mild pain in the right hypochondrium, and cardiopulmonary examination was unremarkable. The patient denied sexual intercourse in the past year. Blood test examination on day 1 showed a normal white blood cells (WBC) count 9,600 cells/uL (neutrophils 61%, lymphocytes 23%), mild increase in C-reactive protein (CRP) 3.22 mg/dL, elevated liver enzyme with aspartate transaminase (AST) 63 U/L, alanine transaminase (ALT) 98 U/L, total bilirubin 3.06mg/dL (direct bilirubin 2.7), γ-glutamyl transferase 579 U/L and alkaline phosphatase (ALP) 1362 U/L. Then, a point-of-care abdominal ultrasound was performed and it was unremarkable. On day 2, the patient had a sudden onset of dyspnea, tachypnea (respiratory rate 24 breaths per minute), and decreased oxygen saturation SpO2 90% in room air. The arterial blood gas analysis showed respiratory alkalosis due to respiratory failure with pH 7.48, pO2 55 mmHg, pCO2 35 mmHg, and the patient required oxygen supplementation with Venturi Mask (VM) 35% followed by an increase of peripheral oxygen saturation (SpO2 96%). Microbiological examinations and a pulmonary CT scan with intravenous contrast were required. The CT scan (Figure 1) excluded pulmonary embolism but showed multiple millimetric rounded nodular lesions in both lungs (suspected for mycotic foci, secondary lesions, or other). Some hypotheses in differential diagnosis were excluded, i.e. pulmonary amyloidosis and sarcoidosis in the absence of risk factors or cryptococcosis and AIDS-related Kaposi sarcoma given the persistent good immune-virological status, septic pulmonary embolism was excluded after a negative echocardiogram. However, the patient’s respiratory distress had induced us to start on day 2 antibiotic therapy with ceftriaxone 1g i.v.
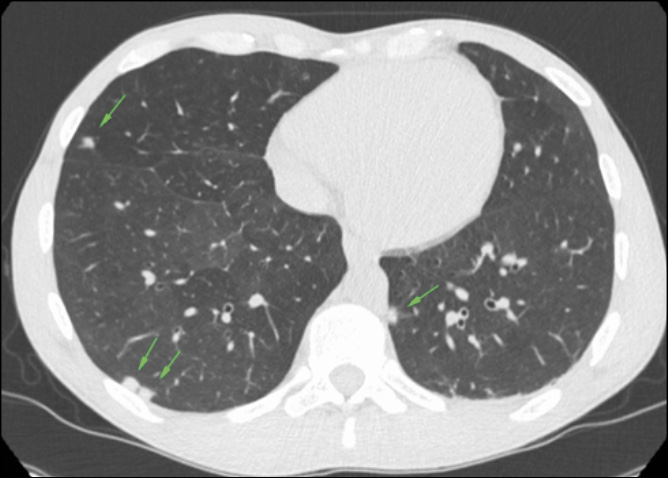
Figure 1 - Pulmonary CT scan on day 2, showing millimetric rounded nodular lesions on both lungs (green arrows).
We performed a wide range of microbiological tests and all turned out negative: a respiratory panel film array on nasal swab (for viruses and bacteria causing common pneumonia), urinary Legionella and Pneumococcus Antigens, Interferon Gamma Release Assay (IGRA) test, serum beta-D-glucan and galactomannan, Widal-Wright reaction, IgM/IgG Rickettsia . Given these data, we excluded most of the common causes of pneumonia. HIV viral load on day 2 was not detected, CD4+ count was >600 cells/µL (31%) with a CD4+/CD8+ ratio 0.7. Serology for syphilis turned out positive: RPR 1:32 and TPPA 1:40,960. After a brief literature research, we noticed that in some cases, syphilitic pneumonia may present with nodular lesions. So we decided to search Treponema pallidum DNA on bronchoalveolar lavage (BAL) in addition to more common pneumonia pathogens. On day 6 the following microbiological tests on bronchoalveolar lavage (BAL) were performed: culture for bacteria/fungi, PCR and Ziehl-Neelsen for mycobacteria, galactomannan, Aspergillus DNA, Pneumocystis jirovecii DNA, film array panel for virus/bacteria. All these results were negative, except for Treponema pallidum DNA, that turned out positive. So, antibiotic therapy was switched on intramuscular Benzylpenicillin 2.4 MU daily. However, after 4 days of ceftriaxone therapy, we had noticed an improvement in blood test with reduction in inflammatory markers (CRP 3 mg/dL, AST 44 U/L, ALT 64 U/L, total bilirubin 1.46 mg/dL) and an improvement in respiratory performance (on day 6, the patient’s saturation was 98% in VM 24%). This could be related to the fact that ceftriaxone is also a second line therapy for syphilis. On day 10 the patient was discharged with a normal oxygen saturation level in room air, CRP 2.1 mg/dL, AST 53 U/L, ALT 82 U/L, alkaline phosphatase 792 U/L, GGT 300, bilirubin 1.03 mg/dL. Due to mild elevation in liver enzymes seven days course of doxycycline 100mg bid was prescribed. Three months after discharge, the patient performed a follow-up blood test examination that was unremarkable, as well as HIV-RNA and CD4+ count, and serology for syphilis that showed a negative RPR and a reduced TPPA 1:5,120 and a pulmonary CT scan that showed a volumetric reduction of the nodular lesions on both lungs (Figure 2).
Followed procedures were in accordance with Helsinky Declaration and an informed consent was obtained by the patient.
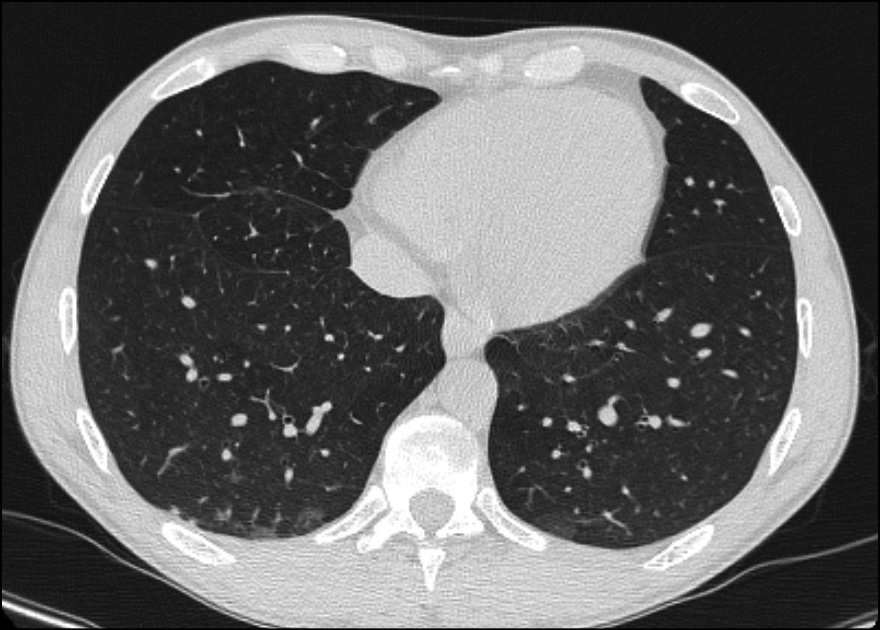
Figure 2 - Pulmonary CT scan performed 3 months after discharge showed a volumetric reduction of the nodular lesions on both lungs.
LITERATURE REVIEW
Methods
A systematic search was performed without language restrictions using Pubmed combining the terms ((Pulmon* OR Pneum*) AND (syphil*)) displaying results until June 1, 2024. All references listed were furthermore hand-searched for relevant articles.
We included articles written in English language, in which authors reported a case of confirmed syphilis with radiologic evidence of pulmonary involvement. We excluded cases with only clinical diagnosis, without radiologic and serologic evidences. Cases involving congenital syphilis were excluded. The following variables were considered: age, gender, pre-existent conditions, risk factors, HIV serology status, clinical presentation (if there was cutaneous rash, fever, weight loss, night sweats, cough, pleuritic pain, and dyspnea), syphilis serology status, the type of radiologic exam and its findings, the therapeutic regimen, clinical outcome and radiological findings at follow up (if any).
The systematic review followed PRISMA (Preferred Reporting Items for Systematic Review and Meta-Analysis) guidelines. The selected articles were reviewed by 3 independent reviewers (A.G., M.A., G.P.). Discrepancies between reviewers were discussed with a different reviewer. A statistical analysis was conducted by G.P., using SPSS © v.29 (Figure 3).
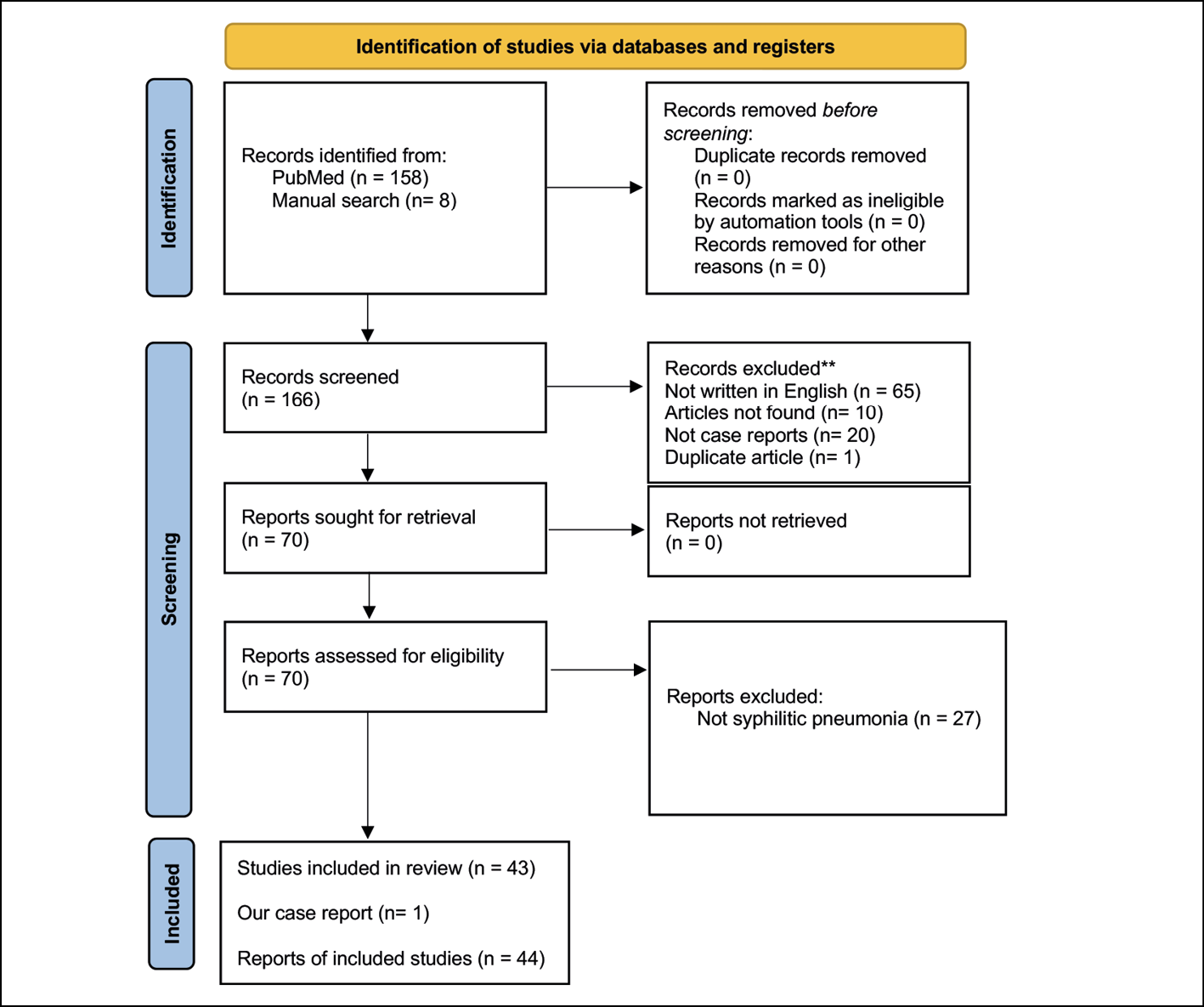
Figure 3 - PRISMA flow chart with study retrieval and selection process.
Results
In our review, we included 43 case reports and added our case. The first description of syphilitc pneumonia was reported in 1886 in a 30-year-old male in a Calcutta Hospital (India), but it was not included in the present review because the diagnosis was based only on clinical criteria and it did not fill our inclusion criteria [6].
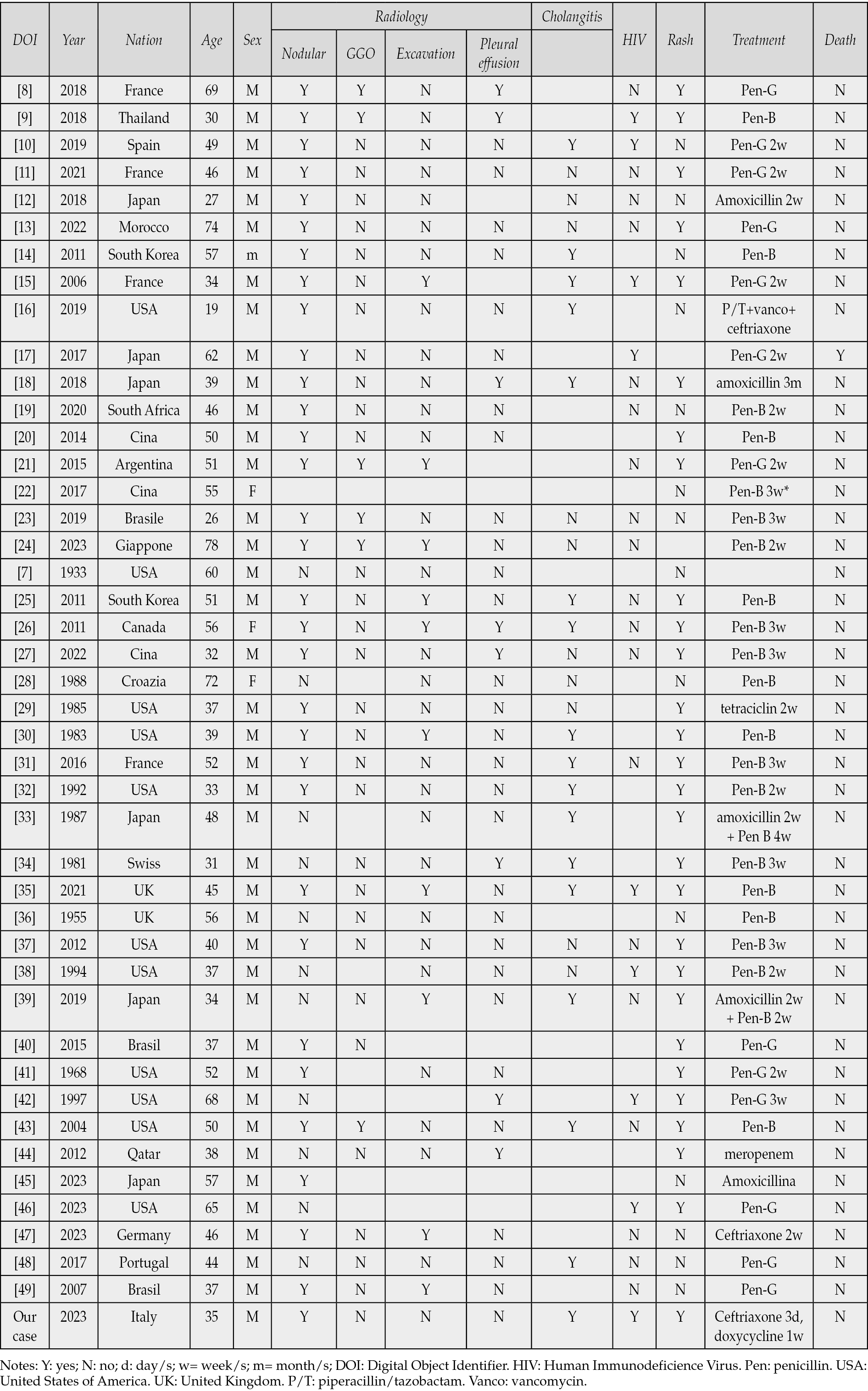
We collected relevant information such as demographic data, sex, age, HIV infection, treatment, outcome, radiographical appearance and the presence of a skin rash (Table 1). Only 1/44 (2.3%) patients died during hospitalization, a 19-year-old male, with hypersexual and bipolar disorders, with unknown HIV status who died 24 hours after admission. The favorable outcome of the other 43/44 (97.7%) patients demonstrated the low mortality rate of secondary form of syphilis and a good response to penicillin.
Table 1 - Overview of all available similar cases in the literature, relevant information, treatment, and outcome.
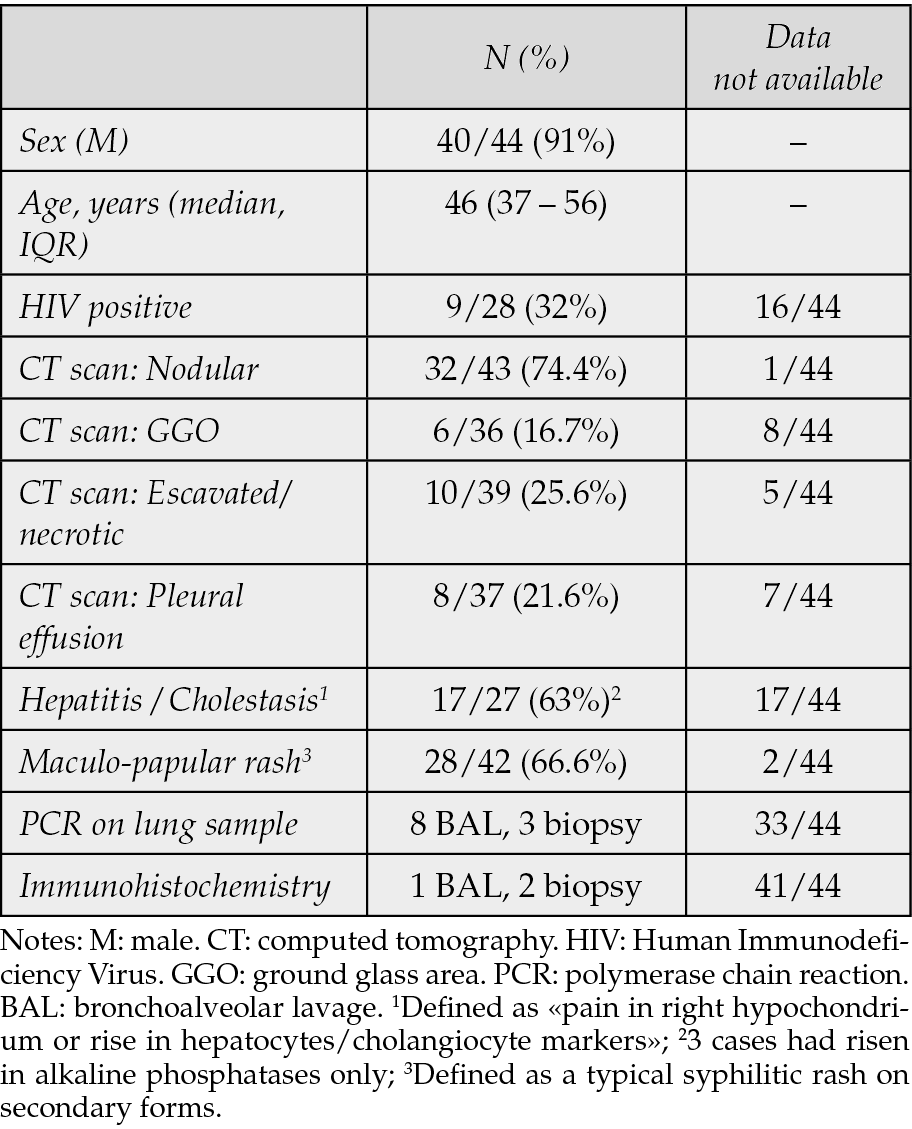
Results are summarized in Table 2. Most patients 40/44 (91%) were male, with a median age of 46 years (37-56, IQR range 25%-75%). HIV patients were 9/28 (32%), but unfortunately, 16/44 did not perform the test for HIV. The high rate of male (91%) among patients with syphilitic pneumonia, could be a consequence of the higher prevalence of syphilis in males. Very interesting is the higher rate of nodular lesions on chest-X ray or CT scan 32/43 (74.4%) which could be defined as a specific pattern for syphilitic pneumonia, despite finding ground-glass opacities areas 6/36 (16.7%) and excavated or necrotic areas 10/39 (25.6%). In two-thirds of the cases, there were observed other manifestations of secondary syphilis, such as maculopapular rash in 28/42 (66.6%) and hepatitis or cholestasis in 17/27 (63%).
Positive PCR for T. pallidum was found on BAL in 8 patients and on pulmonary biopsies in 3 cases; positive immunohistochemistry on BAL for 1 patient and on biopsies for other 2 patients.
Table 2 - Demographic data and clinical data from literature review.
Histologically, on biopsies, syphilitic pneumonia is characterized by the presence of granulomas or lymphoplasmacytic infiltrates. Even epithelioid cell granulomas occur occasionally in secondary syphilis, especially in the late stage, and less frequent is the presence of T. pallidum on biopsy.
Syphilitic pneumonia should be considered in the differential diagnosis of atypical pneumonia cases, even though it is a rare secondary form of syphilis.
We would like to focus on the diagnostic challenges in our case. The nodular lung involvement is an infrequent presentation of typical and atypical pneumonia (caused by viruses or bacteria) and even of metastatic spread (septic or neoplastic). In our case we were induced to widen our ethiological hypotheses because of the complex presentation (well defined nodular lesions, skin rash, cholestatic hepatitis without gallbladder lithiasis) in a patient with several risk factors (PLWH, MSM, although he denied recent sexual intercourse).
The diagnosis is often challenging due to the nonspecific nature of the symptoms and the rarity of the condition, and sometimes it could be observed in tertiary forms making differential diagnosis even more difficult. In our review, nodular pneumonia is the most common radiological finding, with or without excavation.
Rounded nodular lesions should be addressed to many infectious and non-infectious diseases, such as: septic pulmonary embolism, viral, bacterial, or fungal pneumonia, mycobacterial pneumonia, but also sarcoidosis or amyloidosis, osteosarcoma metastases, AIDS-related Kaposi sarcoma, pulmonary lymphoma. These diseases must be considered in the differential diagnosis.
In 1983 Diana Lewis Coleman and colleagues tried to define criteria for syphilitic pneumonia shedding light on a so far unrecognized disease [30]. Authors hypothesized 5 criteria to define syphilitic pneumonia: ”a history and physical findings of typical secondary syphilis; serological test results positive for syphilis; exclusion of other forms of pulmonary disease when possible by findings of serological tests, sputum smears and cultures and cytological examination of sputum; therapeutic response to anti-syphilitic treatment visible on a radiograph; pulmonary abnormalities seen on radiographs with or without associated pulmonary symptoms or signs”. Given the results of our review, with a 74.4% of nodular findings on radiological examination, we would like to suggest one modification for the criteria for syphilitic pneumonia, on the “radiological criteria”: as “pulmonary abnormalities, particularly in the presence of nodular lesions on chest X-ray or pulmonary CT scan, with or without associated pulmonary symptoms or signs”.
Furthermore, we treated our patient with a second-line therapy (due to a delayed diagnosis) and we observed a mild but constant improvement. However, we would like to remember that the first-line therapy is a penicillin-based therapy, and that a different treatment could lead a partial or a non-response. Finally, we may consider that a delayed diagnosis (in terms of month or years) could lead to a worse or even a fatal outcome.
Since syphilis is known as “the great imitator”, atypical syphilis manifestation should always be considered, in particular in immunocompromised patients. Some authors reported atypical syphilitic cutaneous manifestations (nodular, annular, pustolar, psoriasiform rash) up to 25% of cases, mainly in people with VDRL > 1:32 [50].
CONCLUSIONS
Syphilitic pneumonia is a well-known secondary form of syphilis. Diagnosis poses a wide range of differential diagnoses if the patient has only a pulmonary involvement. However, history, serology, and physical findings of syphilis could guide clinicians in the diagnosis. Furthermore, pulmonary rounded nodular lesions on chest X-ray or pulmonary CT scan should be considered as a typical pattern for pulmonary syphilis, and molecular tests on lung tissue or bronchoalveolar lavage may help to confirm the disease.
Finally, we suggest clinician to keep attention on sexually transmitted diseases, especially in at-risk populations with cutaneous rash (although mild and non-well defined) and/or cholestatic hepatitis (with a lithiasis-free gallbladder). Health authorities should improve the screening protocols for syphilis in these populations, and clinicians should pay attention to atypical pneumonia presentations in these populations: physician should also think of “zebras” [51].
Conflicts of interest
Authors declare no conflicts of interest.
Funding
This research received no external funding.
An informed consent was obtained by the patient.
Author contributions
Conceptualization, GP and CIa; methodology, GP and AC; validation, CIa and AC; data curation, GP, AG and MA; writing - original draft preparation, GP, AG, MA; writing, review and editing, AC, CIa; visualization, GP, MA AG, CB, FGM, CIm, GC, ALS, GGM, D.M., AC, CIa; supervision, AC and CI; All authors have read and agreed to the published version of the manuscript.
REFERENCES
[1] Control CfD. Sexually Transmitted Infections Surveillance, 2022 2024 [Available from: https://www.cdc.gov/std/statistics/2022/default.htm.
[2] Malincarne L, Angeli G, Francisci D, Baldelli F, Pasticci MB. Trend of syphilis among patients at the Infectious Diseases Clinic of Perugia, Italy: a six-year observational retrospective study. Infez Med. 2013; 21(1): 14-20.
[3] Foggia M, Gentile I, Bonadies G, et al. A retrospective study on HIV and syphilis. Infez Med. 2014; 22(1): 26-30.
[4] Ciccarese G, Di Biagio A, Drago F, et al. Monkeypox virus infection mimicking primary syphilis. Infez Med. 2022; 31(1): 113-115.
[5] Amer FA, Hammad NM, Wegdan AA, ElBadawy NE, Pagliano P, Rodriguez-Morales AJ. Growing shreds of evidence for monkeypox to be a sexually transmitted infection. Infez Med. 2022; 30(3): 323-327.
[6] Pal B. Calcutta Police Hospital: Syphilitic Paraplegia-Pleuro-Pneumonia. Ind Med Gaz. 1886; 21(10): 299-300.
[7] Ellman P. Syphilitic Aortitis and Diffuse Pulmonary Fibrosis. Proc R Soc Med. 1933; 27(1): 22-25.
[8] Kassem Youssef H, Blind A, Chouta Ngaha F, Drenou B, Nojavan H, Michel C. Secondary pulmonary syphilis: Case report and review of literature. Ann Dermatol Venereol. 2018; 145(4): 278-287.
[9] Visuttichaikit S, Suwantarat N, Apisarnthanarak A, Damronglerd P. A case of secondary syphilis with pulmonary involvement and review of the literature. Int J STD AIDS. 2018; 29(10): 1027-1032.
[10] Hermida-Lama E, Marco-Hernandez J, Medaglia AA, et al. Cholangitis and pulmonary nodules in a clinical presentation of syphilis in an HIV-infected patient. Int J STD AIDS. 2019; 30(8): 820-824.
[11] Benainous R, Alunji M, Brillet PY, Dhote R. Pulmonary Involvement in Secondary Syphilis. Eur J Case Rep Intern Med. 2021; 8(7): 002487.
[12] Komeno Y, Ota Y, Koibuchi T, Imai Y, Iihara K, Ryu T. Secondary Syphilis with Tonsillar and Cervical Lymphadenopathy and a Pulmonary Lesion Mimicking Malignant Lymphoma. Am J Case Rep. 2018; 19: 238-243.
[13] Mougui A, Baba Z, El Bouchti I. Case of Secondary Syphilis with Mucocutaneous, Articular, and Pulmonary Involvement in a 74-Year-Old Moroccan Man. Am J Case Rep. 2022; 23: e937513.
[14] Kim HJ, Seon HJ, Shin HH, Choi YD. Case report: Pulmonary syphilis mimicking pulmonary hematogenous metastases on chest CT and integrated PET/CT. Indian J Radiol Imaging. 2011; 21(1): 34-37.
[15] David G, Perpoint T, Boibieux A, et al. Secondary pulmonary syphilis: report of a likely case and literature review. Clin Infect Dis. 2006; 42(3): e11-e15.
[16] Sharma S, Mehta A. A Case of Pulmonary Syphilis Resulting in Multi-organ Dysfunction and Consequential Demise of a 19-Year-old Male. Cureus. 2019; 11(9): e5560.
[17] Ogawa Y, Imai Y, Yoshihara S, et al. Pulmonary involvement of secondary syphilis. Int J STD AIDS. 2018; 29(1): 89-91.
[18] Ohta A, Furusyo N, Kishihara Y, et al. Secondary Syphilis with Pulmonary Involvement. Intern Med. 2018; 57(1): 121-126.
[19] Govender D, Jackson C, Chetty D. Syphilitic Pulmonary Inflammatory Pseudotumor: A Diagnostic Challenge. Int J Surg Pathol. 2021; 29(1): 90-96.
[20] Fu Z, Zhang J, Li Q, Liu M, Kang L. A case of secondary syphilis involving tonsil, pulmonary, and multiple lymph nodes: 18F-FDG PET/CT findings. Clin Nucl Med. 2015; 40(4): 335-337.
[21] Riganti J, Martin M, Torre AC, et al. Secondary syphilis with pulmonary involvement. J Eur Acad Dermatol Venereol. 2016; 30(12): e177-e179.
[22] Zhao L, Xu X, Zhang Y, Li S, Shi X, Cui Y. Primary lung carcinoma combined with pulmonary amyloidosis secondary to syphilis infection. J Thorac Dis. 2018; 10(2): E145-E148.
[23] Florencio KBV, Costa ADD, Viana TCM, Gomes DCA, Gouveia P. Secondary syphilis with pulmonary involvement mimicking lymphoma: a case report. Rev Soc Bras Med Trop. 2019; 52: e20190044.
[24] Goda K, Katsurada M, Doi T, Saga N, Maniwa Y, Kenzaka T. Pulmonary syphilis with a cicatricial variant of organizing pneumonia: a case report. BMC Pulm Med. 2023; 23(1): 170.
[25] Kim SJ, Lee JH, Lee ES, et al. A case of secondary syphilis presenting as multiple pulmonary nodules. Korean J Intern Med. 2013; 28(2): 231-235.
[26] McCready JB, Skrastins R, Downey JF, Powis JE. Necrotic pulmonary nodules in secondary syphilis. CMAJ. 2011; 183(3): E163-E166.
[27] Yang X, Wu W, Wang Y, Wu W, Huang X, Xu L. A Case of Secondary Pulmonary Syphilis - The Utility of mNGS in Bronchoalveolar Lavage Fluid: A Case Report. Infect Drug Resist. 2022; 15: 5215-5219.
[28] Jankovic S, Mise K, Alujevic A, Tocilj J, Marasovic D, Andjelinovic S. A case of syphilitic interstitial pulmonary fibrosis. Croat Med J. 1998; 39(4): 453-454.
[29] Geer LL, Warshauer DM, Delany DJ. Pulmonary nodule in secondary syphilis. Australas Radiol. 1985; 29(3): 240-242.
[30] Coleman DL, McPhee SJ, Ross TF, Naughton JL. Secondary syphilis with pulmonary involvement. West J Med. 1983; 138(6): 875-878.
[31] Jeny F, Fargelat A, Laurent-Roussel S, et al. Pulmonary Consolidations due to Secondary Syphilis with Positive Bronchial Washing Immunohistochemistry. Am J Respir Crit Care Med. 2016; 193(9): 1061-1062.
[32] Cholankeril JV, Greenberg AL, Matari HM, Reisner MR, Obuchowski A. Solitary pulmonary nodule in secondary syphilis. Clin Imaging. 1992; 16(2): 125-128.
[33] Kurumaji Y, Katoh T, Ohtaki N, Tachibana S, Hashimoto K. A case of secondary syphilis with a solitary pulmonary lesion. Dermatologica. 1987; 174(1): 23-27.
[34] Schibli H, Harms M. Tumour-like pulmonary lesion in secondary syphilis. A case report. Br J Vener Dis. 1981; 57(6): 367-371.
[35] Bell N, Bracchi M, Pozniak A. A case of pulmonary nodules in a patient living with HIV diagnosed with secondary syphilis. BMJ Case Rep. 2021; 14(8).
[36] Knight GH, Fowler W. Peripheral neuritis associated with a pulmonary lesion in a patient with syphilis. Br J Vener Dis. 1955; 31(3): 175-178.
[37] Alrajab S, Payne K, Areno J, Holladay R, Smith T, Zhang S. A 40-year-old man with a nodular lung disease and skin rash. Chest. 2012; 141(6): 1611-1617.
[38] Dooley DP, Tomski S. Syphilitic pneumonitis in an HIV-infected patient. Chest. 1994; 105(2): 629-631.
[39] Futami S, Takimoto T, Nakagami F, et al. A lung abscess caused by secondary syphilis - the utility of polymerase chain reaction techniques in transbronchial biopsy: a case report. BMC Infect Dis. 2019; 19(1): 598.
[40] Soares Souza A, Jr., Soares Souza A, Zanetti G, Marchiori E. A skin rash with multiple pulmonary nodules. Eur Respir Rev. 2015; 24(138): 682-683.
[41] Biro L, Hill AC, Kuflik EG. Secondary Syphilis With Unusual Clinical and Laboratory Findings. JAMA. 1968; 206(4): 889-891.
[42] Zaharopoulos P, Wong J. Cytologic diagnosis of syphilitic pleuritis: a case report. Diagn Cytopathol. 1997; 16(1): 35-38.
[43] Olson AL, Gutman JA, Welsh CH. A 50-year-old man with skin lesions and multiple pulmonary nodules. Chest. 2004; 125(6): 2322-2327.
[44] Elzouki AN, Al-Kawaaz M, Tafesh Z. Secondary syphilis with pleural effusion: case report and literature review. Case Rep Infect Dis. 2012; 2012: 409896.
[45] Arisawa Y, Sugawara K, Morioka H, Takada K. Syphilis Showing Multiple Pulmonary Nodules without Respiratory Symptoms. Intern Med. 2024; 63(6): 885-886.
[46] Johnston AD, Roy SF, McNiff J, Petrazzuoli M. Granulomatous secondary syphilis with pulmonary involvement. JAAD Case Rep. 2024; 44: 23-26.
[47] Angerer M, Lubbersmeyer F, Gubitz R, Wulfing C, Dieckmann KP. Tertiary Syphilitic Gumma Mimicking Testicular Neoplasms. Cureus. 2023; 15(4): e37392.
[48] Freitas DMM, Azevedo A, Pinheiro G, Ribeiro R. Psoriasiform papules, condyloma lata, lung nodules and hepatitis: the enormous variability of secondary syphilis manifestations. BMJ Case Rep. 2017; 2017.
[49] Rocha-Filho JA, Gasparetto EL, Lopes de Oliveira EV, Soares Souza A, Jr., Marchiori E. [Secondary syphilis with pulmonary involvement: report of a case with emphasis to the high-resolution CT and magnetic resonance findings]. Rev Port Pneumol. 2007; 13(5): 737-740.
[50] Ciccarese G, Facciorusso A, Mastrolonardo M, Herzum A, Parodi A, Drago F. Atypical Manifestations of Syphilis: A 10-Year Retrospective Study. J Clin Med. 2024; 13(6).
[51] Ghanem KG, Ram S, Rice PA. The Modern Epidemic of Syphilis. N Engl J Med. 2020; 382(9): 845-854.