Le Infezioni in Medicina, n. 4, 532-537, 2024
doi: 10.53854/liim-3204-12
CASE REPORTS
Pasteurella multocida prosthetic joint infection. A case report and review of the literature
Maria Lagadinou1,2, Panagiotis Antzoulas3, Georgios Eleftherakis1, Christodoulos Chatzigrigoriadis2, Marina Amerali1, Christos Michailides1, Petros Zampakis2,4, Leonidia Leonidou1, Markos Marangos1,2
1Department of Internal Medicine, University Hospital of Patras, Patras, Greece;
2Medical School of Patras, Faculty of Health Sciences, University of Patras, Patras, Greece;
3Department of Orthopedics, University Hospital of Patras, Patras, Greece;
4Radiology Department, University Hospital of Patras, Patras, Greece
Article received 13 May 2024 and accepted 30 September 2024
Corresponding author
Maria Lagadinou
E-mail: mlagad@upatras.gr
SummaRY
Pasteurella multocida is a Gram-negative coccobacillus that is a part of normal oral flora of animals, especially cats and dogs. It is the most common causative agent for soft tissue infections following a bite or scratch from domestic pets. Prosthetic Joint Infections (PJIs) due to Pasteurella multocida are rarely but increasingly reported. Since 1992, only a few cases of PJIs caused by P. multocida have been described. Herein we present a case of a 67-year-old immunocompetent elderly female who developed total hip arthroplasty infection due to P. multocida and was treated successfully with left hip washout, pseudo-tumor removal, and intravenous antibiotics and a review of the literature on prosthetic joint infections caused by P. multocida since 1992.
Keywords: Prosthetic join infections, Pasteurella multocida, debridement.
INTRODUCTION
Prosthetic joint infections (PJIs) are typically associated with aerobic bacteria such as Staphylococci, Streptococci, and Enterococci, while Gram-negative bacilli are less commonly isolated pathogens [1]. However, PJIs due to Pasteurella multocida are rarely but increasingly reported. Since 1992, only a few cases of PJIs caused by P. multocida have been described.
Pasteurella multocida is a Gram-negative coccobacillus that is a part of normal oral flora of animals, especially cats and dogs. It is frequently responsible for soft tissue infections in humans, usually following a bite or scratch from domestic pets Involvement of bones or joints is a rare complication, while infection of a prosthetic joint is even more infrequent [2, 3].
We present a case of P. multocida Total Hip Arthroplasty (THA) infection and a review of the literature on PJI caused by P. multocida over the last 22 years.
CASE PRESENTATION
A 67-year-old female presented to the emergency department with diarrhea, pain, swelling, and pronounced erythema of her left foot extending just below the knee. The patient had undergone total left hip arthroplasty (THA) 10 years prior due to degenerative hip osteoarthritis. She reported a cat bite on her left foot occurring just two days before admission. On arrival, the patient was febrile, with a temperature of up to 39ºC. Her vital signs showed a heart rate of 110 bpm and a blood pressure of 100/82 mmHg. The left leg (lower third of the tibia) was warm, swollen, and erythematous, with a tense effusion and severely restricted range of motion due to pain.
The chest X-ray was normal, with no hilar lymphadenopathy observed. Standard hip radiography was satisfactory and did not show any obvious alterations around the implant (Figure 1). The patient’s white blood cell count was 17.2×109/L with a neutrophilia (14.2 × 109/l), C-reactive protein (CRP) of 20mg/l (<0.5 mg/l), thrombocytopenia, elevated fibrinogen (478 mg/dl), and elevated high-sensitive troponin (1893 ng/dl), which was attributed to Type II ischemia, which further refers to a form of ischemia associated conditions that cause an imbalance between myocardial oxygen supply and demand. The patient was initially administered piperacillin - tazobactam and daptomycin intravenously (i.v). Due to persistent pain which extended above the knee the next days, the patient underwent Magnetic Resonance Imaging (MRI) (Figure 2a-e). MRI showed large encapsulated multilobular fluid collection with internal septa adjacent to the endoprosthesis of the left hip joint (Figure 2a-2b). This collection extended anteriorly beneath the deep fascia, causing displacement of the quadriceps muscle and protruding into the iliopsoas pouch. Its maximum outer diameter measured 12 cm.
The collection exhibited heterogeneous content, peripheral enhancement, as well as solid-enhancing wall components (Figure 2c-2d). Moreover, bilateral myositis was noted in the upper thigh muscle groups, with abscess formation in the left rectus femoris and the left vastus lateralis (Figure 2e). These findings suggested the presence of an inflammatory pseudotumor following hip arthroplasty, possibly compounded by systemic bacteremia, as evidenced by a history of cat bite. Fluid accumulation was also evident in the pelvic cavity.
Of the three blood cultures that were sent to the lab, Pasteurella multocida was isolated in one. Based on these findings, the patient was scheduled for surgical treatment, which was performed within a week. She underwent a left hip washout and pseudotumor removal under general anesthesia. She continued for two weeks receiving intravenously piperacillin-tazobactam and daptomycin (in the case of coexistence of a Gram-positive organism that was not isolated) after surgery completing a total period of one month. The patient was discharged with orally antibiotic treatment (ciprofloxacin and clindamycin) for two weeks. Follow-up appointments were scheduled monthly for the first six postoperative months. The patient was asymptomatic at last follow-up.

Figure 1 - AP X-Ray of the Left Hip Join: Findings compatible with Total Hip Arhtroplasty. No obvious alteration around the implant for example: no loosening signs.
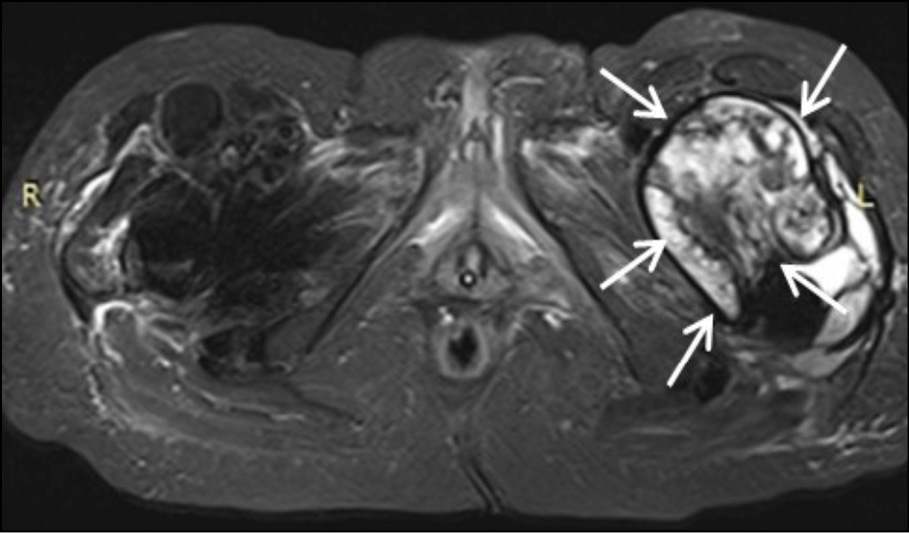
Figure 2a - Axial STIR image at the level of femoral neck. Large encapsulated multilobular fluid collection with internal septa is observed adjacent to the endoprosthesis of the left hip joint (white arrows).
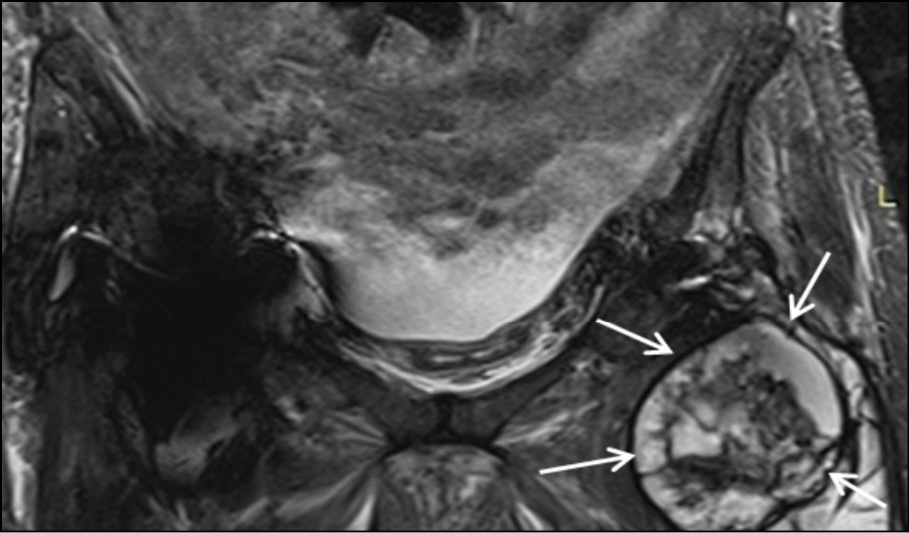
Figure 2b - Coronal STIR image at the level of pubic bone. Large encapsulated multilobular fluid collection with internal septa is depicted adjacent to the endoprosthesis of the left hip joint (white arrows).
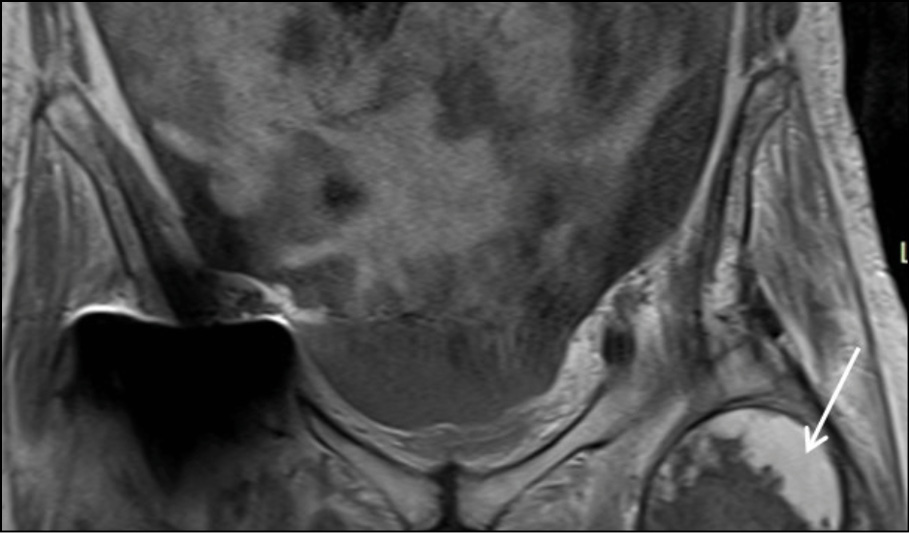
Figure 2c - Coronal T1 post Gd Fat –Suppression image at the level of pubic bone. White arrow shows the peripheral enhancement of the encapsulated collection.
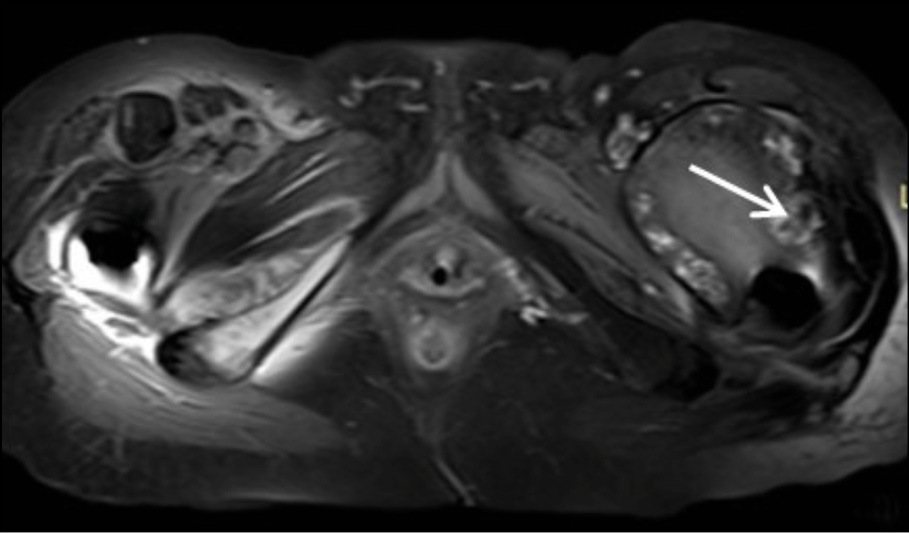
Figure 2d - Axial T1 post Gd Fat –Suppression image at the level of femoral neck. White arrow shows the peripheral enhancement of the encapsulated collection.
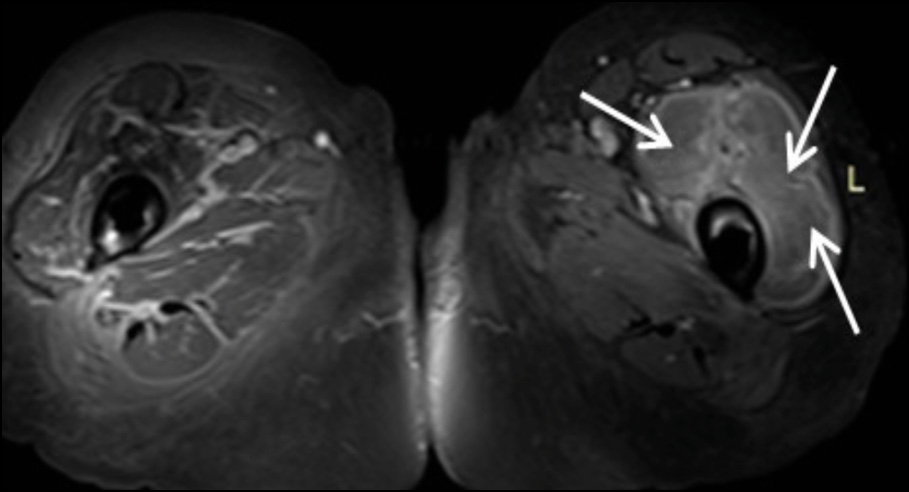
Figure 2e - Axial T1 post Gd Fat –Suppression image at the level of proximal femur. White arrow shows abscess formation in the left rectus femoris and the vastus laterali.
LITERATURE REVIEW
A literature search of the case reports was performed in PubMed and in Google Scholar. The criteria were “Total Hip Arthoplasty (THA) infection due to Pasteurella multocida” and “Total Knee Arthroplasty (TKA) infection due to Pasteurella multocida”. The keywords used in our search were “Pasteurella multocida”, “Prosthetic joint infection”, “ΤΗΑ infection due to P. multocida” and “ΤΚΑ infection due to P. multocida”.
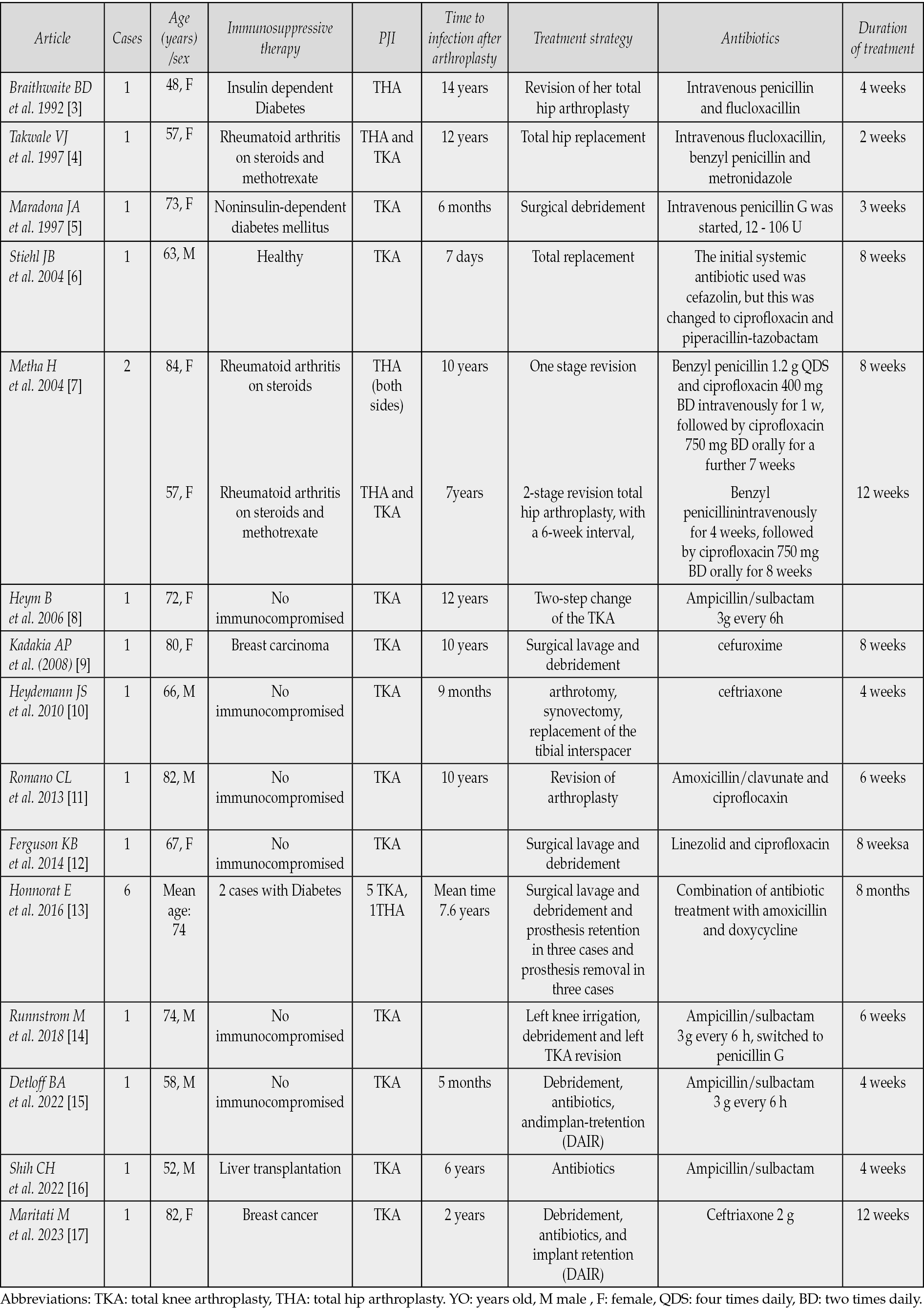
Search results were limited to articles written in the English-language. There were 14 publications; 6 were found in PubMed and 8 in Google Scholar (the first one was reported in 1992 and the last one was reported in 2023) (Table 1) [3-17]. Out of the 21 cases, most were male, with an average age of 68 years. The majority had total knee arthroplasty. Most patients underwent surgical replacement combined with beta-lactam antibiotics (ampicillin-sulbactam, amoxicillin, piperacillin/tazobactam).
Table 1 - Publications of Pasteurella multocida prosthetic join infections.
DISCUSSION
Total Hip Arthroplasty (THA) and Total Knee Arthroplasty (TKA) are highly effective procedures that significantly improve patients’ quality of life [18]. However, Prosthetic Joint Infections (PJIs) following total joint arthroplasty represent a challenging and rare complication for orthopedic surgeons. Given that hip and knee replacements are among the most frequently performed and successful surgeries worldwide, and considering the substantial proportion of the population that owns pets, PJIs present an elevated risk for patients..
The most common causative pathogen remains Staphylococcus aureus reported in up to 34% of cases, followed by coagulase-negative staphylococci and streptococci while Gram-negative species are rarely isolated [19-20]. Pasteurella multocida is a well-known opportunistic pathogen of the oral flora of dogs and cats, as well as a nasopharyngeal and respiratory flora. Since 1992, only 21cases of PJIs caused by P. multocida have been described, as it is well presented in Table 1. P. multocida is the causative pathogen of skin and soft tissue infections and, more rarely, septic arthritis, osteomyelitis, prosthetic joint infections (PJIs), peritonitis, pneumonia, endocarditis, sepsis, and meningitis, particularly in immunocompromised hosts [3, 7, 14-15]. Mehta and Mackie reported that patients with prosthetic joints, particularly if immunocompromised, should be warned that cat and dog bites and cat scratches are potential sources of infection [4, 7]. Strong clinical suspicion is needed so that they should seek urgent medical attention and even receive antibiotic chemoprophylaxis [2, 4]. Maradona et al. suggest the administration of antibiotic prophylaxis in patients who have suffered a pet bite and have a prosthetic joint or Rheumatoid Arthritis or have undergone corticosteroid therapy [5]. American Academy of Pediatrics (AAP), Infectious Diseases Society of America (IDSA) and American Academy of Family Physicians (AAFP) support the use of broad-spectrum prophylactic antibiotics for 3-5 days as soon as possible (within 12-24 hours) after a pet (dog and cat) bite under certain circumstances which apply for the majority of patients. All patients with prosthetic joint must receive antibiotic prophylaxis after a pet bite in combination with wound care, tetanus prevention [2, 4, 5, 7].
We present a case of an immunocompetent elderly female who developed a P. multocida infection in a total hip arthroplasty following a cat bite below her left knee. Notably, infections from licks and scratches often occur distal to the prosthetic joint without direct trauma to the joint itself [14, 17]. Patients are predominantly female, and PJIs most commonly involve a single joint, typically the knee. Over 50% of patients with PJIs have altered host defenses such as female sex, rheumatoid arthritis, obesity, kidney disease, diabetes mellitus, corticosteroid use, alcoholism, organ transplants, COPD, malignancy, multiple surgeries, abnormal intraoperative bleeding, postoperative hematoma, prolonged postoperative drainage, and advanced age [4, 5, 7, 8, 10-12, 14, 15, 17]. Our patient had only two of these risk factors: female gender and older age.
Treatment of P. multocida joint infections includes surgical options and antibiotic treatment. If treated with antibiotics, the treatment includes penicillins, fluoroquinolones, and second or third-generation cephalosporins. It is important to note that while most human isolates remain susceptible to beta-lactams, strains isolated from animals have demonstrated marked resistance to a variety of antibiotics [21]. Furthermore Martina Maritati et al reported the first case of a Drug-Resistant Pasteurella multocida Prosthetic Knee infection successfully treated with debridement, antibiotics, and implant retention [17]. Many patients still require surgical debridement or joint replacement in addition to antibiotics. Joint replacement is done in either one step or two step procedures.
In conclusion, this case underscores several important points related to the diagnosis and treatment of Pasteurella-related joint infections. It is well mentioned that is more than typical a history of animal exposure, that cat bite-related infections may appear earlier, and the decision to perform an exchange arthroplasty is multifactorial and depends on the severity of the infection. Strong clinical suspicion is essential for patients with domestic animals and prosthetic joints who present with symptoms of septic arthritis.
Authors’ contribution
ML, PA and GE conceptualized the work and treated the patient, ML, CC,MA, CM, PZ, GE, PA, LL reviewed the literature and wrote the paper, MM supervised and edited the paper.
Funding
No grants or funding were received.
Conflicts of interest
The authors declare that there are not any conflicts of interest.
Availability of data and materials
Available upon reasonable request.
Ethics approval
This case report was conducted in line with the Helsinki Declaration.
Consent of publication
The patient gave consent for publication
REFERENCES
- Zardi EM, Franceschi F, Prosthetic joint infection. A relevant public health issue. J Infect Public Health. 2020; 13(12): 1888-1891.
- Lam PW, Page AV. Pasteurella multocida non-native joint infection after a doglick: A case report describing a complicated two-stage revision and a comprehensive review of the literature. Can J Infect Dis Med Microbiol. 2015; 26(4): 212-217.
- Braithwaite BD, Chir B, Giddins G. Pasteurella multocida infection of a total hip arthroplasty. A case report. J Arthroplasty. 1992; 7(3): 309-310.
- Takwale VJ, Wright ED,Bates J, Edge AJ. Pasteurella multocida infection of a total hip arthroplasty following cat scratch. J Infect. 1997; 34(3): 263-264.
- Maradona JA, Asensi V, Carton JA, Guardado AR, Castellano JL. Prosthetic joint infection by Pasteurella multocida. Eur J Clin Microbio lInfect Dis. 1997; 16(8): 623-625.
- Stiehl JB, Sterkin LA, Brummitt CF. Acute Pasteurella multocida in total knee arthroplasty. J Arthroplasty. 2004; 19(2): 244-247.
- Mehta H, Mackie I. Prosthetic joint infection with Pasteurella multocida following cat scratch: a report of 2 cases. J Arthroplasty. 2004: 19(4): 525-527.
- Heym B , Jouve F, Lemoal M, Veil-Picard A, Lortat-Jakob A, Nicolas-Chanoine MH. Pasteurella multocida infection of a total knee arthroplasty after a “doglick”.Knee Surg Sports Traumatol Arthrosc. 2006; 14(10): 993-997.
- Kadakia AP, Langkamer VG. Sepsis of total knee arthroplasty after domestic cat bite: should we warn patients? Am J Orthop. 2008; 37(7): 370-371.
- Heydemann J, Heydemann JS, Antony S.Acuteinfection of a total knee arthroplasty caused by Pasteurella multocida: a case report and a comprehensive review of the literature in the last 10 years. Int J Infect Dis. 2010; 14(Suppl. 3): e242-245.
- Romano CL, De Vecchi E, Vassena C, Manzi G, Drago L.A case of a late and atypical knee prosthetic infection byno-biofilm producer Pasteurella multocida strain identified by pyrosequencing. Pol J Microbiol. 2013; 62(4): 435-438.
- Ferguson KB, Bharadwaj R, MacDonald A, Syme B, Bal AM. Pasteurella multocida infected total knee arthroplasty: a case report and review of the literature. Ann R Coll Surg Engl. 2014; 96(2): e1-e4.
- Honnorat E, Seng P, Savini H, Pinelli PO, Simon F, Stein A. Prosthetic joint infection caused by Pasteurella multocida: a case series and review of literature. BMC Infectious Diseases. 2016; 16(1): 435.
- Runnstrom M, Hyde R, Shah K. Pasteurella multocida prosthetic joint infection. ID Cases. 2018; 13: 4.
- Detloff LR, Atri Ν. Periprosthetic joint infection in bilateral knees caused by Pasteurella multocida. Priv Pract Infect Dis. 2022; 2(4): 14.
- Shih CY, Chen HY. Pasteurella multocida in total knee prosthetic joint infection caused by cat scratches and bites in a liver transplant recipient. ID Cases. 2022; 29: e01560.
- Maritati M, Liverani L, Gigante A, Zanoli GA, De Rito G. The first case of a drug resistant Pasteurella multocida prosthetic knee infection successfully treated with debridement, antibiotics, and implant retention. Cureus 2023; 15(5): e38389.
- Shichman Ι, Roof M, Askew N, Seyler TM, et al. Projections and epidemiology of primary hip and knee arthroplasty in Medicare patients to 2040-2060. JB JS Open Access. 2023; 8(1): e22.00112.
- Izakovicova P, Borens O, Trampuz A. Periprosthetic joint infection: current concepts and outlook. EFORTOpen Rev. 2019; 4(7): 482-494.
- Tsai Y, Chang CH, Lin YC, Lee SH, Hsieh PH, Chang Y. Different microbiological profiles between hip and knee prosthetic joint infections. J Orthop Surg (Hong Kong). 2019; 27(2):
- Kehrenberg C, Schulze-Tanzil G, Martel JL, Chaslus-Dancla E, Schwarz S. Antimicrobial resistance in Pasteurella and Mannheimia: epidemiology and genetic basis. VetRes. 2001; 32(3-4): 323-339.