Le Infezioni in Medicina, n. 2, 264-266, 2024
doi: 10.53854/liim-3202-15
LETTER TO THE EDITOR
MERS outbreak in Riyadh: A current concern in Saudi Arabia
Vasso Apostolopoulos1, Vivek Chavda2, Najim Z. Alshahrani3, Rachana Mehta4,5, Prakasini Satapathy5,6 , Alfonso J. Rodriguez-Morales7,8,*, Ranjit Sah9,10,11
1Institute for Health and Sport, Victoria University, Werribee Campus, VIC 3030, Australia;
2Department of Pharmaceutics and Pharmaceutical Technology, L M College of Pharmacy, Ahmedabad, Gujarat, India;
3Faculty of Medicine, University of Jeddah, Jeddah, Saudi Arabia;
4Dr Lal PathLabs Nepal, Chandol, Kathmandu, Nepal;
5Medical Laboratories Techniques Department, AL-Mustaqbal University, 51001 Hillah, Babil, Iraq;
6Center for Global Health Research, Saveetha Medical College and Hospital, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai, India;
7Faculty of Health Sciences, Universidad Científica del Sur, Lima, Peru;
8Gilbert and Rose-Marie Chagoury School of Medicine, Lebanese American University, Beirut, Lebanon;
9SR Sanjeevani Hospital, Kalyanpur, Siraha, Nepal;
10Department of Microbiology. D. Y. Patil Medical College, Hospital and Research Centre, Dr. D. Y. Patil Vidyapeeth, Pune, Maharashtra, India;
11Department of Public Health Dentistry, Dr. D. Y. Patil Dental College and Hospital, Dr. D. Y. Patil Vidyapeeth, Pune, Maharashtra, India.
Received 10 May 2024; accepted 22 May 2024
Corresponding author
Alfonso J. Rodriguez-Morales
E-mail: arodriguezmo@cientifica.edu.pe
Dear Editor,
The COVID-19 pandemic, the latest in a series of coronavirus outbreaks, follows in the footsteps of its predecessors: the 2002 Sudden Acute Respiratory Syndrome (SARS) and the 2012 Middle East Respiratory Syndrome (MERS) epidemics [1]. While these outbreaks share virological similarities, they differ significantly in their global impact and severity. Unlike COVID-19, neither SARS nor MERS reached the same scale, yet they posed considerable threats due to their higher case fatality rates (%CFR). SARS, caused by SARS-CoV-1, resulted in a CFR of 11%, claiming 774 lives out of 8,096 reported cases [2]. MERS, caused by MERS-CoV, presents an even graver outcome with a CFR of 36%, accounting for approximately 941 deaths among 2,613 reported cases with the majority being in Saudi Arabia, with 2204 cases and 860 deaths (CFR of 39%) [3]. MERS was first identified in June 2012 in Saudi Arabia, with most cases occurring in the Arabian Peninsula (Bahrain, Iran, Jordan, Kuwait, Lebanon, Oman, Qatar, Saudi Arabia, UAE, and Yemen). Other countries include Algeria, Austria, China, Egypt, France, Germany, Greece, Italy, Malaysia, Netherlands, Korea, Philippines, Thailand, Tunisia, Turkey, the United Kingdom, and the United States of America, of which travel appears to have been the main cause (Figure 1).
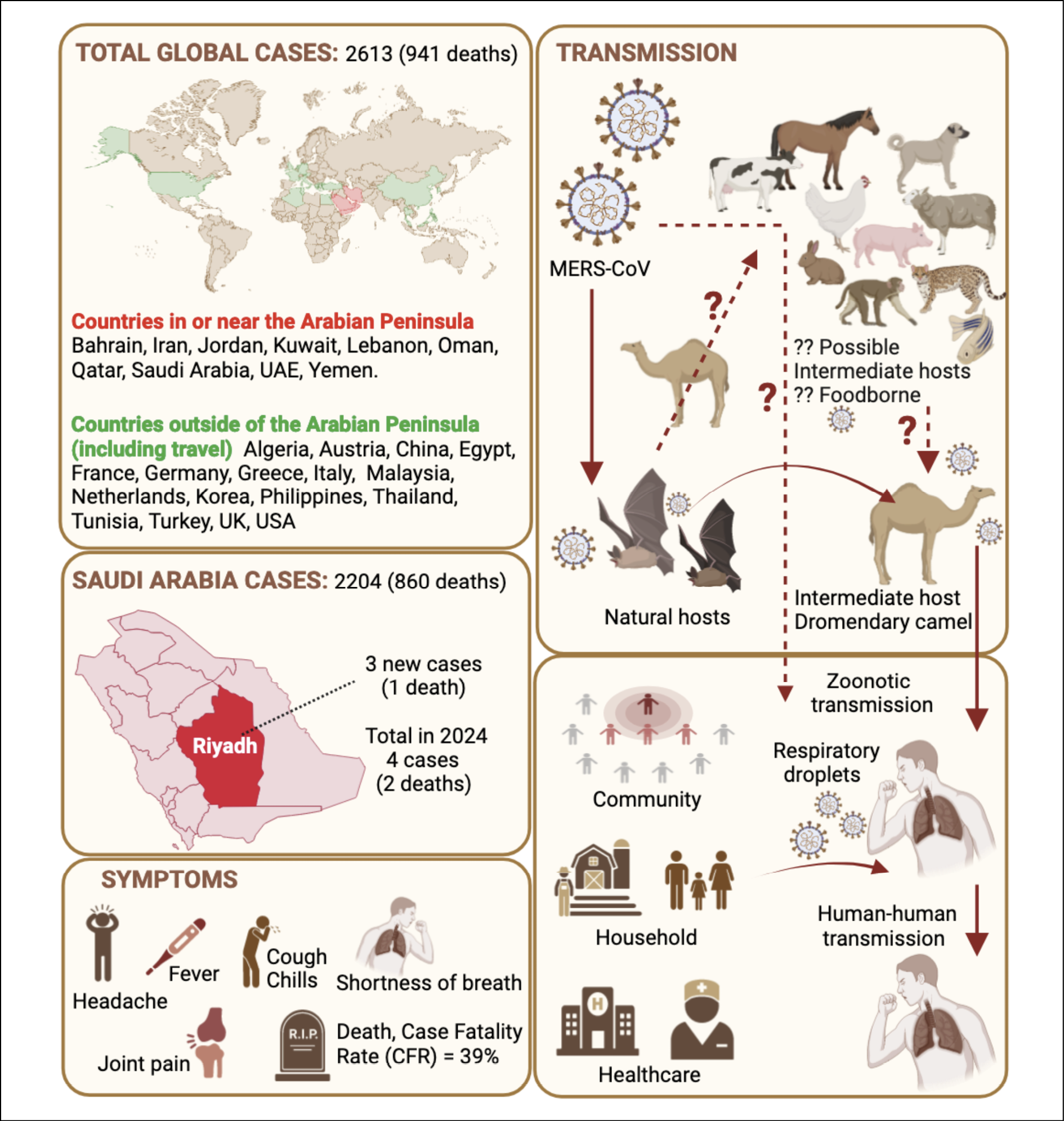
Figure 1 - The current outbreak of Middle East Respiratory Syndrome Coronavirus (MERS-CoV) in Saudi Arabia, in April 2024, comprises 3 reported cases, resulting in 1 fatality. In total for the year 2024, there have been 4 cases and 2 deaths attributed to MERS in Saudi Arabia. Globally, there have been 2613 reported cases of MERS with 941 fatalities, with the majority of cases (2204) and deaths (860) occurring in Saudi Arabia. The Case Fatality Rate (CFR) stands at approximately 39%. Since its identification in 2012 in Saudi Arabia, MERS has been reported in several other countries, including non-Arabian Peninsula nations where cases have been attributed to travel. Symptoms of MERS include headache, fever, cough, chills, shortness of breath, joint pain, and death. Bats are considered natural hosts of MERS-CoV, while dromedary camels serve as intermediate hosts. The figure depicts currently unknown other possible intermediate hosts and possible foodborne transmission (dotted lines). Transmission to humans is primarily zoonotic from camels, and it is believed to occur via respiratory droplets from humans through close contacts such as, community, household, and healthcare settings
Current evidence indicates Arabian camels, or Dromedary camels, are a species of camels native to the Middle East, and they are a primary reservoir for MERS-CoV, though transmission routes are unclear. High titers of neutralising anti-MERS-CoV antibodies have been identified in camels [4]. Antibodies are also being detected in sheep, goats, cattle and chickens. It is unclear at this stage if transmission occurs from other animals or foodborne sources (Figure 1). Although sustained human-to-human transmission is not observed, cases have emerged from close contact, particularly in household, community or healthcare settings [5]. The perceived risk to the global population is currently considered significantly low. Outbreaks, the largest in South Korea, Saudi Arabia, and the UAE, emphasise global concern [6]. Prevention requires avoiding raw animal products, adopting safe hygiene practices near camels and in healthcare settings, and educating the community and healthcare workers. Although efforts have been made, no specific antiviral treatments or vaccines are currently available for MERS-CoV, highlighting the requirement for rigorous control measures and continuous research. Recent publications have shown promising advancements in vaccine and drug design [7, 8]. Currently, treatment is supportive and tailored to the individual symptoms exhibited by the patient, along with isolation, fluid management and respiratory support. To prevent MERS transmission, avoiding handling or consuming raw camel products like milk and urine, undercooked camel meat and thorough handwashing are essential.
In April 2024, the Ministry of Health of Saudi Arabia reported three cases (with one death) of MERS-CoV in Riyadh, with no apparent link to camels and not healthcare workers; all three cases were linked to the same healthcare facility [3]. The first case, a 56-year-old male teacher, was admitted to hospital on 4 April and subsequently tested positive. He was from Riyadh, Saudi Arabia, with underlying health issues and developed symptoms of cough, fever, and body aches, and no precise exposure to typical MERS-CoV risk factors [9]. Two other cases, both males aged 60, with underlying health conditions, were identified through contact tracing, likely due to contact with the first case. Investigations are ongoing to determine the route of transmission. One of the two-second cases shared a room with the original case, while the other was in a different ward. No additional cases were identified among close contacts. As of 21 April 2024, the second and third cases remained in ICU and were intubated. Investigations are ongoing to determine the source of infection and prevent further spread, with follow-up of healthcare workers. Since 16 February 2024, one more case of MERS-CoV was reported, a 32-year-old male from Taif, Saudi Arabia, with camel contact. A total of 4 MERS-CoV cases in Saudi Arabia thus far in 2024 with two deaths. The World Health Organization (WHO) emphasises the importance of quick investigations and the absence of typical MERS-CoV risk factors in affected individuals, highlighting the need for source determination. These recent cases do not alter the overall risk assessment but indicate a likelihood of more infections in the coming weeks to months, with the area facing a ‘high threat’. Vigilance is crucial, given MERS’ ongoing global persistence as a significant danger, including potential future MERS-like outbreaks as potential new pandemic threats [10]. Research and clinical trials are ongoing to develop specific antiviral treatments and vaccines for MERS, but currently, supportive care remains the mainstay of treatment for this viral respiratory illness.
Funding
No funding received
Ethical approval
Not applicable
Conflict of interest
Authors Declare No conflict of interest
Authors contribution
V.A, V. C: Writing original draft, N.Z.A., R.M, P.S, A.J.R.M: writing review and editing, R. S: Supervision.
REFERENCES
[1] Chavda VP, Yao Q, Vora LK, et al. Fast-track development of vaccines for SARS-CoV-2: The shots that saved the world. Front Immunol. 2022; 13: 961198.
[2] Chan-Yeung M, Xu RH. SARS: epidemiology. Respirology. 2003; 8(Suppl. 1): S9-14.
[3] World Health Organisation, Middle East respiratory syndrome. Accessed 12 May 2024.
[4] Hemida MG, Perera RA, Wang P, et al. Middle East Respiratory Syndrome (MERS) coronavirus seroprevalence in domestic livestock in Saudi Arabia, 2010 to 2013. Euro Surveill. 2013; 18(50): 20659.
[5] Assiri A, McGeer A, Perl TM, et al. Hospital outbreak of Middle East respiratory syndrome coronavirus. N Engl J Med 2013; 369(5): 407-416.
[6] Mohapatra RK, Padhi BK, Kandi V, et al. Camel virus (MERS) reported from Qatar: a threat to the FIFA-2022 and Middle East. QJM. 2023; 116(2): 150-152.
[7] Biswas S, Mita MA, Afrose S, et al. An in silico approach to develop potential therapies against Middle East Respiratory Syndrome Coronavirus (MERS-CoV). Heliyon. 2024; 10(4): e25837.
[8] Chao CW, Sprouse KR, Miranda MC, et al. Protein nanoparticle vaccines induce potent neutralizing antibody responses against MERS-CoV. bioRxiv. 2024.
[9] MERS outbreak in Saudi Arabia puts health experts on high alert The Telegraph Access 10 May 2024.
[10] Zumla A, Peiris M, Memish ZA, Perlman S. Anticipating a MERS-like coronavirus as a potential pandemic threat. Lancet. 2024; 403(10438): 1729-1731.