Le Infezioni in Medicina, n. 3, 440-445, 2022
doi: 10.53854/liim-3003-13
ORIGINAL ARTICLES
Adherence to antiretroviral therapy thought package-refill among HIV+ persons at “D. Cotugno” hospital, Naples, Italy
Francesco Maria Fusco, Nadia Sangiovanni, Nunzia Papa, Nunzia Cuomo, Orsola Tambaro, Valentina Iodice, Vincenzo Bruner, Maria Aurora Carleo, Viviana Rizzo, Giulia Palmiero, Mariana Di Lorenzo, Micaela Spatarella, Rosaria Viglietti, Vincenzo Sangiovanni, Vincenzo Esposito
“D. Cotugno” Hospital, AOS dei Colli, Naples, Italy
Article received 29 April 2022, accepted 3 July 2022
Corresponding author
Francesco M. Fusco
E-mail: francescomaria.fusco@ospedalideicolli.it
SummaRY
Background: A gold-standard for the measurement of adherence to antiretroviral therapy (ART) is lacking. Aim of this study is to verify the feasibility of a package-refill-based measurement of ART at “D. Cotugno” hospital, Naples, Italy, and the factors associated to adherence.
Methods: In the period January 2018-August 2020, we calculated the package-refill as the ratio between ART-packages actually withdrawn, and the ART packages needed to regularly take ART. Adherence was associated, trough a univariate e multivariate logistic regression, to demographical, behavioural and clinical factors.
Results: 1140 HIV+ subjects were included. At univariate logistic regression inadequate package-refill-based adherence is associated with HIV-RNA higher than 50 copies/mmL (OR 3.77-IC95% 2.76-5.13) and with HIV-RNA higher than 200 copies/mmL (OR 3.98-IC95% 2.69-5.90). Being not-Italian and Injective-drug-user are associated with low adherence, having HIV/AIDS for more than 8 years is associated with better adherence.
Conclusions: Package-refill is a suitable method for measuring adherence and is associated with the condition of viral failure.
Keywords: antiretroviral therapy, adherence, package-refill, HIV/AIDS.
INTRODUCTION
Adherence to antiretroviral therapy (ART) is one of the major determinants of sustained HIV virologic suppression, restoration of immune system, prevention of drug resistance and reduced risk of HIV transmission [1, 2]. On the other side, studies suggest that long-term adherence is difficult to maintain and tools for the appropriate monitoring of adherence are needed, in order to promptly identify patients with poor adherence [3].
There is no gold standard for estimating ART adherence and several methods have been proposed. Most used methods to assess ART adherence in randomized controlled trials have included patient self-report, electronic monitoring and pill count [4]. In real-life, other methods have included pharmacy refill data, communication instruments such as SMS-recall and assessing pharmacologic drug levels in biological samples. Most feasible and acceptable measure may change place by place, based on the local organization and resources.
Pharmacy-based measures include pill-refill count and/or package-refill count. These measures are based on the ratio between the number of pills/packages actually withdrawn compared to those that should have been withdrawn to ensure optimal adherence. These measures have several advantages: the assessment of pill/package refills is not expensive, easy to conduct, since data are already included in pharmacy records and may provide an overall long-term estimation of adherence [5]. Among these measures, the package-refill is easier to be assessed.
The aim of this study is to verify the overall ART adherence measured through a package-refill-based adherence measure in a large sample of Persons Living With HIV (PLWH) stably followed-up at “D. Cotugno” hospital, Naples, South Italy. As secondary end points, we explored the demographical, behavioural and clinical factors associated to inadequate adherence to ART.
PATIENTS AND METHODS
Study design
This is a retrospective observational study exploring
- the feasibility of a measure for ART adherence monitoring, the package-refill count,
- the adherence to ART and
- the factors associated to inadequate adherence among a population of PLWH in care at “D. Cotugno” hospital, Naples, Southern Italy.
Setting
The study setting is the “D. Cotugno” hospital, a mono-specialistic infectious diseases referral centre sited in Naples, Campania, Southern Italy. Campania is the most populous region in Southern Italy, counting for 6 million of inhabitants. The “D. Cotugno” hospital has a long-term tradition in HIV/AIDS care and some Medical Units are mainly dedicated to in-patient and out-patient management of PLWH. Specific HIV diagnostics are performed within the hospital laboratory. A total of about 2500 PLWH are in care at “D. Cotugno” hospital, accounting for about 70% of PLWH in Campania Region.
Participants and data source
A sample of patients with HIV/AIDS in care at “D. Cotugno” hospital, those referring to 2 HIV/AIDS Units and accounting for 50% of the entire PLWH hospital population, were included in the study. Among the patients selected, only subjects stably in care in the period January 2018-August 2020 were included, defined as patients with at least one access per year for laboratory assessment and at least one access per year for ART package withdraw. Data sources were represented by clinical electronic database for patients’ records, and by pharmacy electronic database for package-refill data.
Variables
The main outcome of the study is represented by ART adherence measured by package-refill. Package refill is calculated as the ratio between ART packages actually withdrawn, compared to the number of ART packages needed to regularly take the therapy. We considered adequate a package-refill ≥95% of packages withdrawn in the study period, partial a package-refill of 70%-94%; inadequate a package-refill less than 70%.
In order to verify the accountability of this measure, we included HIV-RNA in study period as main dependent variable. We classified HIV-RNA as: always less than 50 copies/mmL; at least one record between 51-200 copies/mmL; and at least one record higher than 200 copies/mmL.
Other variables of interest included in the study were: demographical data (age, gender, origin); risk factor for HIV acquisition; clinical data (CD4 count, CDC classification, AIDS event in medical history, years of HIV/AIDS, comorbidities); ART-related data (type of ART, pill burden).
Statistical methods
Package-refill have been calculated as the ratio between the number of packages of ART actually withdrawn in hospital pharmacy compared to the expected number of packages to be withdrawn (32 packages for the period January 2018-August 2020). For patients with first diagnosis (or first referring to Cotugno hospital) during the study period, the number of packages to be withdrawn for the first year were considered as 6 in 2018 and 2019, and 4 packages in 2020.
Statistical differences among frequencies and percentages were calculated with the Student’s Chi-squared test or t student test, as appropriate, using a significance level of 0.05. Factors associated to inadequate adherence were calculated by a univariate and multivariate logistic regression. Data were analysed using the free PSPP software.
RESULTS
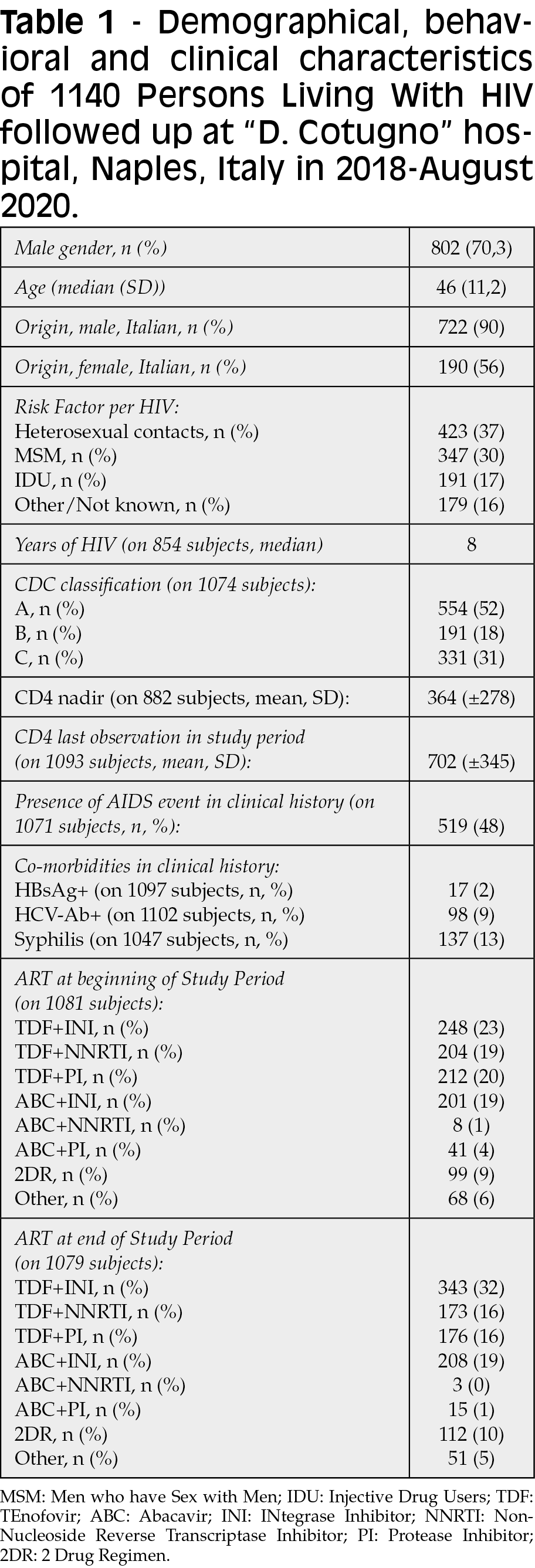
A total of 1210 PLWH were randomly selected and included in the database. Among these patients, those stably in care were 1140, who represent the population included in the study. Demographical, behavioural and clinical characteristics of these PLWH are summarized in Table 1. The population is mainly constituted by males, median age is 46-years-old for both males and females. Patients of foreign origin were 20% of the whole population, foreign origin is more present among female patients (44% of females are not Italian, compared with 10% of males). The population has a long HIV/AIDS history, with median of 8 years of infections. At study time, level of CD4 shows a mean of 702 cell/mmL, but 48% of study population experienced at least one AIDS event in their life. Infective comorbidities are present in a limited extension.
Main study outcome is presented in Table 2. Subjects with inadequate adherence have an increased risk for viral failure, with OR 3.77 (IC95% 2.76-5.13) for having HIV-RNA 50-200 copies/mmL at least one time in study period, and OR 3.98 (IC95% 2.69-5.90) for having HIV-RNA >200 copies/mmL at least one time in study period.
At univariate logistic regression (Table 2), being not-Italian and injective drug users are risk factors for inadequate adherence (OR 4.1, IC95% 3.02-5.55 and OR 2.6, IC95% 1.72-3.93, respectively). Instead, HIV infection for more than 8 years (OR 0.62, IC95% 0.44-0.87), having more than 200 CD4 cells/mmL at last observation of study period (OR 0.31, IC95% 0.18-0.53), and taking ART based on Abacavir + Integrase Inhibitors (ABC+INI, OR 0.43, IC95% 0.20-0.95) are protective factors for inadequate adherence.

A multivariate analysis has been performed including gender, age, and all factors emerged as significant at univariate analysis. Among risk factors, the origin of the patient is confirmed (adjusted OR for having inadequate adherence in not-Italian 3.45, IC95% 2.23-5.35), while being HIV+ for more than 8 years is protective (adjusted OR 0.60, IC95% 0.41-0.88). Moreover, a protective role of female gender (adjusted OR 0.64, IC95% 0.43-0.96) emerges.
DISCUSSION
We explored the applicability and suitability of a package-refill-based measure for ART adherence among a population of PLWH. According to data emerged, this measure is feasible to be applied in clinical settings: it is easy and inexpensive to apply, because records are already available in patients’ clinical records and in hospital pharmacy database. The package-refill measure is easy to calculate and may be routinely applied in clinical practice.
The reliability of this measure is confirmed by the outcomes of other variables associated to adherence: package-refill is able to predict the risk of viral failure. Indeed, prevalence of PLWH with HIV-RNA higher than 50 copies or higher than 200 copies is significantly associated to inadequate adherence measured by package-refill.
This measure has some limits, too. Indeed, package-refill does not reflect daily assumption, and it is not a direct measure of drug ingestion. The estimation over a long period (at least one year) is necessary to obtain accurate adherence measure. In our case, a 32-months-period has been applied in most patients.
The correlation between adherence and viral suppression is demonstrated in several studies, among which some conducted in Italy or involving Italy in a multi-country study [6-9].
On the other hand, adherence measurement is not the only determinant of viral failure. In our study population, 11% of patients has at least one HIV-RNA higher than 200 copies, despite an optimal adherence measured by package-refill. Other reasons, such as drug-to-drug interaction, and resistance to ongoing ART may explain this data.
Some factors are associated to inadequate adherence in our population. Foreign origin and being an IDU as risk factor for HIV are all associated to inadequate adherence. Foreign persons are often associated with poor retention in care and adherence, because of their mobility, and because of frequent health and social marginality [10-12]. Similarly, people who inject drugs have been already described among those group at higher risk for inadequate adherence and poor retention in care [13,14]. The association of low adherence, measured by package-refill, with factors and populations well known to be associated with a poor adherence, confirm the reliability of this measure, again.
In our population, longer HIV/AIDS history is associated with better adherence. This finding, is in contrast with other recent finding in other study, where long-term adherence is generally poor [3].
A number of CD4 less or equal to 200 cells/mmL is significantly more present among PLWH with inadequate adherence. This last evidence is probably a consequence of adherence, and not a determining associated factor.
Of note, pill burden is not associated to adherence in our population. PLWH taking a single-tablet-regimen has the same adherence of those taking more than one pill. This finding is common to another Italian study where adherence and related-health status was not different among patients taking qd and bid therapies [8].
Some limitations are present in this study. It is a monocentric study, addressing the half only of entire HIV/AIDS population in care. Moreover, the suitability of the package-refill has been measured in comparison to an outcome, the HIV-RNA level, and not to other adherence measures. The absence of a gold standard for adherence measure is the main reason for this choice.
CONCLUSIONS
Package-refill is a simple and suitable method for measuring adherence, especially is a long-time observation is possible. Factors associated with inadequate adherence in our population is similar to those already described in other adherence studies conducted in Italy.
Authors’ contributions
FMF conceived the study, analyzed data, and drafted the paper; NS collected the data, contributed to draft the paper and to data analysis; NP and NC contributed to data collection and analysis; OT, VI, VB, MAC, VR, MDL, MS, RV contributed to data collection; VS and VE coordinated the study. All authors gave their contribute for important intellectual contents and all authors saw and approved the final version of the manuscript.
Data availability statement
The database of the study is available for review, if required
Funding statement
This study was supported by an unrestricted GILEAD Grant 20200320, N° 10055. Title of the grant: Evaluation of adherence to antiretroviral therapy by measuring the pill-refill and impact on the viro-immunological profile: retrospective data at the D. Cotugno Hospital, period 2017-2019.
Conflict of interest disclosure
All authors declare to have not conflicts of interest about the contents of the study.
Ethics approval statement
Due to the observational nature of the study and the presentation of anonymized aggregated data only, no specific ethic approval has been obtained.
Patient consent statement
For all patients, a generic authorization is obtained to use, exclusively anonymously and collectively, data deriving from clinical practice. This article presents overall data, completely anonymous, from which it is not possible in any way to trace the identity of the subjects involved. For this reason, we have not found it necessary to ask for specific consent.
REFERENCES
- Bangsberg DR, Perry S, Charlebois ED, et al. Non-adherence to highly active antiretroviral therapy predicts progression to AIDS. Aids. 2001; 15 (9), 1181-1183.
- Lima VD, Harrigan R, Bangsberg DR, et al. The combined effect of modern highly active antiretroviral therapy regimens and adherence on mortality over time. J Acquir Immune Defic Syndr. 2009; 50 (5), 529-536.
- Saberi P, Ming K, Legnitto D, Neilands TB, Gandhi M, Johnson MO. Feasibility and acceptability of novel methods to estimate antiretroviral adherence: A longitudinal study. PLoS One. 2019; 14 (1), e0210791.
- Marcellin F, Spire B, Carrieri MP, Roux P. Assessing adherence to antiretroviral therapy in randomized HIV clinical trials: a review of currently used methods. Expert Rev Anti-Infect. 2013; 11 (3), 239-250.
- Saberi P, Chakravarty D, Ming K, et al. Moving antiretroviral adherence assessments to the modern era: correlations among three novel measures of adherence. AIDS Behav. 2020; 24 (1), 284-290.
- de Los Rios P, Okoli C, Punekar Y, et al. Prevalence, determinants, and impact of suboptimal adherence to HIV medication in 25 countries. Prev Med. 2020; 139, 106182.
- Maggiolo F, Di Filippo E, Comi L, et al. Reduced adherence to antiretroviral therapy is associated with residual low-level viremia. Pragmat Obs Res. 2017; 8, 91-97.
- Gianotti N, Galli L, Bocchiola B, et al. Number of daily pills, dosing schedule, self-reported adherence and health status in 2010: a large cross-sectional study of HIV-infected patients on antiretroviral therapy. HIV Med 2013; 14 (3), 153-160.
- Aloisi MS, Arici C, Balzano R, et al. Behavioral correlates of adherence to antiretroviral therapy. J Acquir Immune Defic Syndr. 2002; 31 (Suppl. 3), S145-148.
- Taylor BS, Reyes E, Levine EA, et al. Patterns of geographic mobility predict barriers to engagement in HIV care and antiretroviral treatment adherence. AIDS Patient Care STDS. 2014; 28 (6), 284-295.
- Been SK, van de Vijver DA, Nieuwkerk PT, et al. Risk Factors for Non-Adherence to cART in Immigrants with HIV Living in the Netherlands: Results from the ROtterdam ADherence (ROAD) Project. PLoS One. 2016; 11 (10), e0162800.
- Woolley I, Bialy C. Visiting friends and relatives may be a risk for non-adherence for HIV-positive travellers. Int J STD AIDS. 2012; 23 (11), 833-834.
- Davis A, McCrimmon T, Dasgupta A, et al. Individual, social, and structural factors affecting antiretroviral therapy adherence among HIV-positive people who inject drugs in Kazakhstan. Int J Drug Policy. 2018; 62: 43-50.
- Chan PY, Joseph MA, Des Jarlais DC, Uusküla A. Perceived effectiveness of antiretroviral therapy, self-rated health and treatment adherence among HIV-positive people who inject drugs in Estonia. Int J STD AIDS. 2018; 29 (1), 13-22.