Le Infezioni in Medicina, n. 3, 393-401, 2021
doi: 10.53854/liim-2903-10
ORIGINAL ARTICLES
Clinical profile, management and outcome of patients with leptospirosis during the times of COVID-19 pandemic: A prospective study from a tertiary care centre in South India
Nitin Gupta1,2, William Wilson3, Prithvishree Ravindra3, Sowmya Joylin1, Rachana Bhat3, Kavitha Saravu1,2
1Department of Infectious Diseases, Kasturba Medical College, Manipal Academy of Higher Education, Manipal, Karnataka, India;
2Manipal Center for Infectious Diseases, Prasanna School of Public Health, Manipal Academy of Higher Education, Manipal, Karnataka, India;
3Department of Emergency Medicine, Kasturba Medical College, Manipal Academy of Higher Education, Manipal, Karnataka, India
Article received 17 April, 2021; accepted 28 June, 2021
Corresponding author
Nitin Gupta
E-mail: nityanitingupta@gmail.com
SummaRY
Leptospirosis is a rodent-borne acute febrile illness, classically seen after heavy rainfall and floods. This study aimed to describe the clinical profile, management strategies and outcome of patients with leptospirosis amidst the Coronavirus disease-2019 outbreak.
A prospective study of adult patients with undifferentiated fever (5-15 days) was conducted in South India between October 2020 and February 2021. The demographic, clinical details, laboratory details, treatment and outcome of leptospirosis positive (based on serology) and negative patients were compared. A chi-square test was used for qualitative variables, while an independent t-test or Mann Whitney U test was used for continuous variables.
Of the 206 patients with suspected acute febrile illness, a total of 63 patients were diagnosed with leptospirosis based on serology results. The median sequential organ failure assessment score was higher in those with leptospirosis (p<0.001). Myalgia, abdominal pain, jaundice, decreased urine output, myocarditis, and dialysis requirement were more common in patients with leptospirosis. Leucocytosis and raised procalcitonin/ C-reactive protein were more common in patients with leptospirosis. The duration of stay and antibiotic consumption was higher in patients with leptospirosis.
Acute febrile illness such as leptospirosis should be suspected in tropical areas with significant risk factors. The presence of conjunctival suffusion, hepatic and renal dysfunction should warrant a serology test for leptospirosis.
Keywords: Leptospira, Coronavirus disease 2019, acute febrile illness, tropical infections.
INTRODUCTION
Besides the direct impact of Coronavirus disease 2019 (COVID-19) on mortality, collateral damage includes difficulties in diagnosing and managing neglected diseases such as acute febrile illnesses (AFI). This is predominantly due to the clinical overlap and the majority of clinical and preventive machinery focusing on COVID-19 [1]. AFIs are a common cause of morbidity and mortality in low and middle-income countries like India [2]. Malaria, dengue, scrub typhus, leptospirosis, and enteric fever are responsible for most AFI-related presentations in hospitals across India [3, 4]. Leptospirosis is a widespread zoonotic disease with a significantly higher burden in tropical countries. The most crucial animal reservoirs responsible for transmission are rodents [5]. The rodents transmit the infection to humans by contaminating water sources with their urine containing leptospires [5]. Leptospirosis is endemic in many coastal areas of India, including the states and union territories of Tamil Nadu, Maharashtra, Kerala, Karnataka and Andaman Nicobar Islands [6-13]. Still, large outbreaks have been described following increased rainfall leading to floods, presumably because of the increased risk of exposure to contaminated water. This study describes the clinical features, treatment and outcome of patients with leptospirosis during the COVID-19 pandemic. The study was a part of a diagnostic trial designed to study the impact of rapid diagnostic tests in reducing hospital stay [14].
A prospective study was conducted in a tertiary care teaching hospital located in the coastal district of Udupi (Karnataka, South India) between the 9th of October, 2020 and the 15th of February, 2021. The study was conducted after taking consent from the Institute’s Ethical Committee. Adult patients (more than 18 years of age) with an undifferentiated fever of 5-15 days duration were screened on the working days for enrollment. Those patients with an established microbiological diagnosis or a single localized source of infection at presentation were excluded. All patients were tested for leptospirosis using Lepto IgM Microlisa (J. Mitra, India) or Leptocheck WB (Tulip Diagnostics, India) [15]. The tests were interpreted according to the manufacturer’s instructions. The patients were also tested for dengue, scrub typhus and malaria. Investigations for other relevant etiologies were done according to the hospital policy and physician’s discretion.
The demographic, clinical and laboratory details of all the patients were entered in a clinical case record form. The gender, age (in years), the month of presentation, and comorbidities were recorded for all the patients. History of fever, headache, fatigue, myalgia and symptoms suggestive of systemic involvement was noted. General physical examination details comprising rash, icterus, conjunctival congestion, and organomegaly were also recorded. The haematological and biochemical parameters of all the patients were noted. Acute kidney injury was defined as an increase in serum creatinine by >0.3 mg/dl within 48 hours or increased serum creatinine to >1.5 times the baseline. Oliguria was described as a urine volume of <0.5 ml/kg/hour for six hours. Those patients with electrocardiographic or echocardiographic changes along with elevated troponin were classified as myocarditis. All patients’ treatment details, including number and type of antibiotics, daily defined dosage (DDD) and days of therapy (DOT), were recorded. The antibiotics used were also classified according to the AWaRe classification (Access, Watch and Reserve) established by the World Health Organization (WHO) [16]. The outcome (death or alive) at day 30 from the time of admission was also recorded.
Data analysis: The analysis was done using SPSS v25 (SPSS Inc, Chicago, USA). The data were summarized as the frequency with percentage for categorical data and mean (+ standard deviation) and median (interquartile range) for continuous data. The patients were divided into two groups based on serology results for leptospirosis: leptospirosis positive and leptospirosis negative. They were compared for clinical profile, treatment and outcome. A chi-square test was used for qualitative variables, while an independent t-test or Mann Whitney U test was used for continuous variables. A p-value of <0.05 was considered significant.
RESULTS
A total of 206 patients with suspected AFI of 5-15 days fever were enrolled. The mean duration of fever was 6.1+2. The following co-morbidities were present: diabetes mellitus (n=56), hypertension (n=46), chronic lung disease (n=7), HIV (n=4), hepatitis B (n=3) and malignancy (n=2). The median sequential organ function assessment (SOFA) score at enrollment was 4 (2-7) days. The mean number of antimicrobials used in the enrolled patients was 2.5+1.2. The median number of antibiotics used from the Access and Watch group was 1 (1-1) and 1 (1-2), respectively. A total of 14 (6.8%) patients died during the 30 days of follow-up from the time of admission.
A total of 63 patients were diagnosed with leptospirosis, while leptospirosis serology was negative in 143 patients. The final diagnosis of all patients has been summarized in Figure 1. The seasonal distribution of patients in the two groups has been summarized in Table 1. The median SOFA score was 9 (6-11) in patients with leptospirosis, while it was 5 (3-10) in patients without leptospirosis. The difference was significant (p<0.001). Myalgia, abdominal pain and decreased urine output were more common in patients with leptospirosis, while fatigue, cough and dyspnoea were less common (Table 2). Conjunctival suffusion and icterus were more commonly seen in patients with leptospirosis (Figure 2). Myocarditis, AKI and the requirement for dialysis were higher in patients with leptospirosis. Leucocytosis, raised procalcitonin and raised C-reactive protein (CRP) were more common in patients with leptospirosis, while leucopenia was less common in patients with leptospirosis (Table 3). The median levels of total bilirubin, direct bilirubin, creatinine, procalcitonin and CRP were higher in patients with leptospirosis. The duration of stay was significantly higher in patients with leptospirosis. The antibiotic consumption was significantly higher in patients with leptospirosis (Table 4). The outcome was similar in both groups.
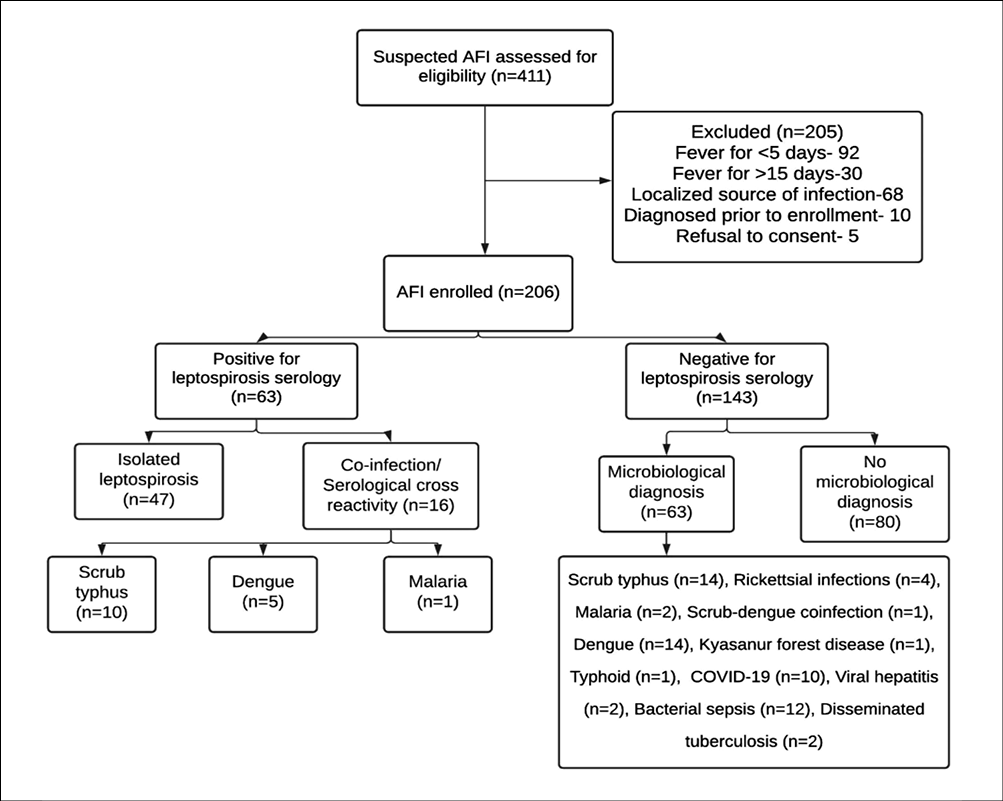
Figure 1 - Screening, enrollment and diagnosis of patients with suspected leptospirosis.
Table 1 - Month-wise distribution of enrolled patients diagnosed with or without leptospirosis.
|
Month of presentation |
Leptospirosis positive (n=63) |
Leptospirosis negative (n=143) |
p-value |
|
October |
11 (17.5%) |
8 (5.6%) |
<0.001 |
|
November |
28 (44.4%) |
20 (14%) |
|
|
December |
17 (27%) |
39 (27.3%) |
|
|
January |
6 (9.5%) |
56 (39.2%) |
|
|
February |
1 (1.6%) |
20 (14%) |
Table 2 - Demography and clinical features of patients diagnosed with or without leptospirosis.
|
Clinical features |
Leptospirosis positive (n=63) |
Leptospirosis negative (n=143) |
p-value |
|
Age (in years) |
48.3 |
45 |
0.152 |
|
Male gender |
45 (71.4%) |
101 (70.6%) |
0.965 |
|
Diabetes mellitus |
9 (14.3%) |
47 (32.9%) |
0.006 |
|
Hypertension |
15 (23.8%) |
31 (21.7%) |
0.735 |
|
Fatigue |
24 (38.1%) |
76 (53.1%) |
0.046 |
|
Headache |
14 (22.2%) |
30 (21%) |
0.841 |
|
Myalgia |
34 (53.9%) |
41 (28.7%) |
0.001 |
|
Arthralgia |
5 (7.9%) |
16 (11.2%) |
0.477 |
|
Rash |
3 (4.8%) |
7 (4.9%) |
0.967 |
|
Bleeding |
2 (3.2%) |
2 (1.4%) |
0.395 |
|
Diarrhoea |
13 (20.6%) |
23 (16.1%) |
0.428 |
|
Abdominal pain |
25 (39.7%) |
35 (24.5%) |
0.029 |
|
Ascites |
18 (28.6%) |
34 (23.8%) |
0.465 |
|
Hepatomegaly |
18 (28.6%) |
34 (23.8%) |
0.465 |
|
Splenomegaly |
11 (17.5%) |
31 (21.7%) |
0.489 |
|
Icterus |
37 (58.7%) |
30 (21%) |
<0.001 |
|
Cough |
5 (7.9%) |
31 (21.7%) |
0.016 |
|
Dyspnoea |
5 (7.9%) |
27 (18.9%) |
0.044 |
|
Chest pain |
2 (3.2%) |
4 (2.8%) |
0.889 |
|
Conjunctival suffusion |
18 (28.6%) |
8 (5.6%) |
<0.001 |
|
Pleural effusion |
2 (3.2%) |
14 (9.8%) |
0.1 |
|
Pericardial effusion |
2 (3.2%) |
1 (0.7%) |
0.174 |
|
Myocarditis |
20 (31.7%) |
25 (17.5%) |
0.024 |
|
Acute kidney Injury |
48 (76.2%) |
55 (38.5%) |
<0.001 |
|
Decreased urinary output |
40 (63.5%) |
41 (28.7%) |
<0.001 |
|
Acute respiratory distress syndrome |
8 (12.7%) |
13 (9.1%) |
0.44 |
|
Dialysis |
15 (23.8%) |
15 (10.5%) |
0.013 |
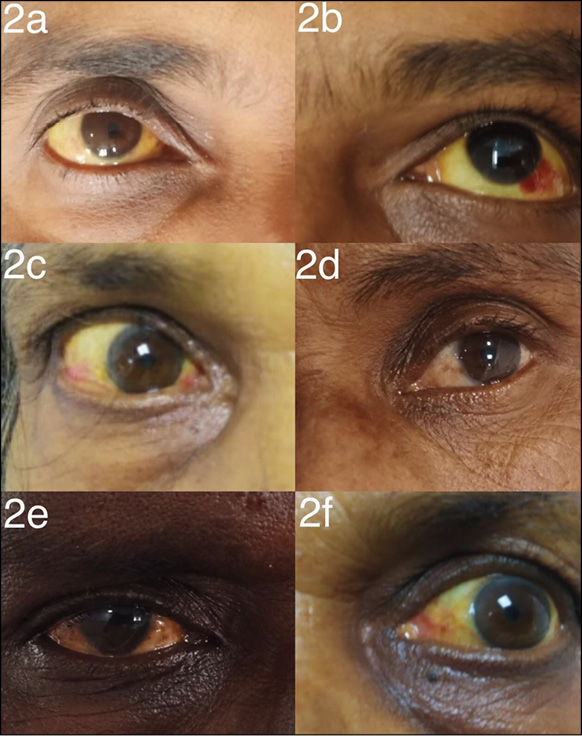
Figure 2 - Eyes of six patients with leptospirosis showing icterus and/or conjunctival suffusion.
Table 3 - Laboratory features of patients diagnosed with or without leptospirosis.
|
Laboratory parameters |
Leptospirosis positive (n=63) |
Leptospirosis negative (n=143) |
p-value |
|
Anaemia |
19 (30.1%) |
30 (21%) |
0.154 |
|
Leucocytosis (>11,000/ cu.mm) |
40 (63.5%) |
63 (44%) |
0.010 |
|
Leucopenia (<4,000/cu.mm) |
5 (7.9%) |
32 (22.4%) |
0.013 |
|
Thrombocytopenia (<1,50,000/cu.mm) |
49 (77.8%) |
97 (67.8%) |
0.148 |
|
Total bilirubin |
4.54 (1.26-13.5) |
1.13 (0.58-3) |
<0.001 |
|
Direct bilirubin |
3.7 (0.7-12) |
0.58 (0.26-2.34) |
<0.001 |
|
Aspartate transaminase |
81 (57-150) |
68.5 (29-145.25) |
0.062 |
|
Alanine transaminase |
58 (40-87) |
57.5 (26-123.5) |
0.618 |
|
Alkaline phosphatase |
141 (110-219) |
128 (79.8-228.2) |
0.274 |
|
Creatinine |
5.41 (1.74-6.68) |
1.55 (0.94-3.26) |
<0.001 |
|
Procalcitonin |
7.76 (2.75-20.4) |
3.13 (1-15.3) |
0.001 |
|
C-reactive protein |
206.9 (102.8-275.1) |
170.8 (79.8-262.1) |
0.001 |
|
Raised Procalcitonin (>0.5 ng/ml) |
52/55 (94.5%) |
78/115 (67.8%) |
0.000 |
|
Raised C-reactive protein (6 mg/dl) |
61/61 (100%) |
119/134 (88.8%) |
0.007 |
Table 4 - Treatment and Outcomes of patients diagnosed with or without leptospirosis
|
Treatment |
Leptospirosis positive (n=63) |
Leptospirosis negative (n=143) |
p-value |
|
Duration of stay |
213 (170-286) |
154 (115-235.5) |
<0.001 |
|
No. of antibiotics |
3 (2-3) |
2 (2-3) |
0.011 |
|
Daily defined dosage |
26 (21-30.66) |
17 (8.3-26.2) |
<0.001 |
|
Days of therapy |
17.5 (14.7-24) |
12 (8-18) |
<0.001 |
|
Penicillin |
10 (15.9%) |
2 (1.4%) |
<0.001 |
|
Ceftriaxone |
55 (87.3%) |
116 (81.1%) |
0.276 |
|
Doxycycline |
57 (90.5%) |
93 (65%) |
0.003 |
|
Azithromycin |
19 (30.1%) |
38 (26.6%) |
0.616 |
|
Piperacillin-tazobactam |
24 (38.1%) |
45 (31.5%) |
0.353 |
|
Meropenem |
4 (6.3%) |
16 (11.2%) |
0.280 |
|
30 Day Final Outcome (Death) |
4 (6.3%) |
10 (7%) |
0.866 |
DISCUSSION
There is a considerable burden of leptospirosis in many parts of India [17]. Leptospirosis is one of the most common causes of admission in the monsoon season in the public and private sectors. There is an increased “out of pocket expenditure” for the patient as well [18]. With the increase in the COVID-19 cases, AFIs have increased the burden on already overburdened hospitals [19]. In a study from Brazil, most leptospirosis clusters occurred after a natural disaster preceded by heavy rainfall in that area [20]. Other studies have described the increased incidence of leptospirosis during monsoon and floods [10, 11, 21-24]. Due to the southwest monsoon winds from July to September 2020, heavy rainfall occurred in Udupi (Karnataka, India) and nearby districts. This led to floods with water entering many houses in the community, thereby increasing the chance of exposure to leptospires [25]. In a study by Temeiam et al., confirmed cases were more likely to have a flooded house [26]. In a report from Sri Lanka, a similar increase in cases of leptospirosis was seen during the COVID-19 pandemic, which was attributed to an increase in agricultural activities during the lockdown and decreased chemoprophylaxis [1]. Apart from isolated case reports, no prospective study on leptospirosis during the COVID-19 pandemic has been published to the best of our knowledge [27].
The clinical course of leptospirosis is variable, with most cases remaining mild, while some are severe and potentially fatal. The existing protocol of isolating all patients with fever in the COVID suspect wards till COVID reports were negative led to a significant delay in diagnosing leptospirosis cases. This explains the high baseline severity in most cases. Similar to previous studies, cases were seen more commonly in men than women [10, 12, 13, 21-24, 28-35]. This might be due to higher chances of exposure during outdoor activities. Most patients present with fever, myalgias, and headache. Myalgia and headache have been described in 28-100% and 19-100% cases respectively in published literature [6, 7, 10, 12, 13, 21, 22, 24, 29, 31, 32, 34-38]. Conjunctival suffusion is characteristically seen in many patients with leptospirosis and may help to make a diagnosis. Its prevalence varies from 1-58% in previously published studies [6, 7, 12, 13, 22, 31, 32, 34, 37]. It was significantly more common in patients with leptospirosis [29%] than other causes of AFI (6%) in our study. Similar to our study, a study from Kerala (India) described muscle tenderness, conjunctival congestion and abdominal pain to be significantly more common in patients with leptospirosis when compared to other AFIs [6]. Hepatic and renal involvement is characteristically described in leptospirosis and is often designated as Weil’s disease. Renal failure is often non-oliguric and reversible, but supportive renal replacement therapy may be required in some cases [39]. Of the 48 leptospira positive patients with AKI, 83% had decreased urine output, and 31% of patients required one or more dialysis sessions. The proportion of oliguria in patients with renal dysfunction varies between study. In the study by Balasundaram et al, of the 54 patients with raised creatinine, 22% of patients had decreased urine output [6]. In another study by Niwattayakul, of the 39 patients with acute renal failure, 50% were oliguric. In the study by Kuriakose et al, 20% had a decrease in urine output while only 16% were classified as renal failure [7]. Other studies have showed the prevalence of AKI and oliguria to be 1-81% and 1-56% respectively [10, 12, 13, 21, 22, 24, 29, 31, 32, 34-36, 38].
Liver involvement is commonly described in patients with leptospirosis. Bilirubin levels were more significantly elevated in patients with leptospirosis (Median-4.5 g/dL) than in other patients with AFI. Similar to previous studies, the levels of transaminases (median AST 81, median ALT 58 IU/mL) were not significantly high. In a previous study, the mean AST and ALT levels were 230 IU/mL and 215 IU/mL [40]. The prevalence of increased bilirubin and elevated transaminases in previous studies have been 14-71% and 45-93% respectively [6, 12, 13, 22, 31, 34, 35, 37]. Leucocytosis was more frequent in patients with leptospirosis, while thrombocytopenia was not different between leptospirosis and other AFIs. A similar finding was shown in another study [6]. The prevalence of leucocytosis in published studies ranged from 33 to 83% [6, 12, 13, 22, 31, 34, 35, 37].
The proportion of leptospirosis patients with raised CRP and procalcitonin was also significantly higher. CRP is an acute-phase reactant that rises rapidly with the onset of inflammation. The levels of CRP are considerably higher in patients with a bacterial infection. In a study from French Guiana, CRP levels were helpful in differentiating dengue and leptospirosis at admission (41). In resource-limited settings, rapid CRP kits may be useful in estimating the requirement of antibiotics in patients with AFI. Similarly, procalcitonin levels are raised in patients with bacterial infections. Although a study reported that procalcitonin levels were consistently high in patients with leptospirosis, to the best of our knowledge, no study has systematically evaluated its utility in differentiating it from other febrile illnesses (42).
Serological tests are used most frequently for the diagnosis of leptospirosis. As most serological tests are positive only after 5-7 days, the study recruited only those with >5 days of illness. Although microscopic agglutination test is the serological gold standard, it is resource-intensive [41]. Several commercial ELISAs are available for making a diagnosis of leptospirosis. In addition, there are many serologically based lateral flow rapid tests also available for the diagnosis of leptospirosis. These tests have been found to have similar diagnostic accuracy to conventional ELISAs. In our study, positivity with either test was taken as positive.
Initial studies showed that penicillin could shorten the duration of illness in patients with leptospirosis [42]. However, a later study in patients with severe leptospirosis showed that penicillin does not improve mortality in patients with more than four days of illness [36]. In a study by Mclain et al., doxycycline reduced the duration of illness when compared to placebo. In another study, ceftriaxone was as effective as penicillin in reducing time to fever resolution [32]. In a study by Suputtamongkol et al, there was no difference between doxycycline, penicillin and cefotaxime with respect to mortality and time to improvement [35]. The use of penicillin, ceftriaxone and doxycycline in different studies range from 34-100%, 28-100% and 8-48% respectively [11, 22, 24, 28, 30, 32, 33, 35, 36, 42-44]. Penicillin, ceftriaxone and doxycycline was used in 16%, 87% and 90% of the patients, respectively. Despite the absence of studies showing the benefit of combination therapy, the median number of antibiotics used in patients with leptospirosis was three in our study. Higher antibiotics like piperacillin-tazobactam and meropenem were also used in significant numbers despite the absence of studies showing significant clinical benefits. The standard duration of therapy for severe cases is seven days, but in our study, the median days of therapy were 17.5, which was significantly higher. The final mortality in patients with leptospirosis was 6%. Previous studies have shown that the mortality with leptospirosis ranges from 2.2-18% [6, 7, 12, 13, 22, 23, 28-32, 36, 37, 45].
To the best of our knowledge, this is the first study during the pandemic that comprehensively compares leptospirosis with other AFIs. Apart from the usual clinical findings such as conjunctival suffusion, jaundice, etc. and laboratory manifestations such as leucocytosis, raised creatinine etc., this study showed raised CRP and procalcitonin can also help differentiate leptospirosis from other causes of AFI. In addition, this study showed that patients with leptospirosis are more severe at presentation, stay for a longer time and are prescribed more antibiotics (number and duration) when compared with other AFIs. This finding is significant as targeted antimicrobial stewardship interventions in patients with leptospirosis may be particularly helpful in decreasing overall antimicrobial consumption.
Acute febrile illness such as leptospirosis should be suspected in tropical areas with significant risk factors. The presence of conjunctival suffusion, hepatic and liver dysfunction should warrant a serology test for leptospirosis. It is of prime importance that the infrastructure and workforce at the healthcare facilities should be expanded to avoid neglect of endemic acute febrile diseases. The primary care physicians should be sensitized about the possibility of AFIs such as leptospirosis amidst the COVID-19 pandemic. The use of appropriate therapy for appropriate duration should be promoted amongst the treating physicians.
Acknowledgements
Departments of Emergency Medicine and General Medicine, Kasturba Medical College, Manipal, India, for their help and support.
Funding
Manipal Centre for Infectious diseases (MAC ID), Manipal Academy of Higher Education, Manipal, India.
Conflicts of interest/competing interests
None.
Authors’ contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Nitin Gupta. The first draft of the manuscript was written by Nitin Gupta, Prithvishree Ravindra and William Wilson. All authors commented on previous versions of the manuscript and were involved in the revision of the first draft. All authors read and approved the final manuscript.
Ethics approval
An ethical approval (IEC/209/2020) was obtained from the Institute’s Ethics committee (Kasturba Medical College and Kasturba Hospital Institutional Ethics Committee) before the initiation of the study. The study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Consent to participate
Informed consent was taken from all participants before enrollment in the study.
Consent for publication
Informed consent for publication was taken from all participants before enrollment in the study.
REFERENCES
- Niriella MA, Ediriweera DS, De Silva AP, Premarathna BHR, Jayasinghe S, de Silva HJ. Dengue and leptospirosis infection during the coronavirus 2019 outbreak in Sri Lanka. Trans R Soc Trop Med Hyg. 2021; Apr 6:trab058.
- John TJ, Dandona L, Sharma VP, Kakkar M. Continuing challenge of infectious diseases in India. Lancet. 2011; 15, 377 (9761), 252-69.
- Gupta N, Nischal N. Management of acute febrile diseases in limited resource settings: a case-based approach. Infez Med. 2020; 1, 28 (1), 11-6.
- Shepard DS, Halasa YA, Tyagi BK, et al. Economic and disease burden of dengue illness in India. Am J Trop Med Hyg. 2014; 91 (6), 1235-42.
- Koizumi N, Morita M, Pheng V, et al. Rat trade and leptospirosis: Molecular epidemiology of Leptospira species in rats exported from Cambodia to Vietnam. Transbound Emerg Dis. 2021; Mar 18. doi: 10.1111/tbed.14077. Online ahead of print.
- Balasundaram PK, Kanakamma LG, Jayageetha K, Selvarajan B. Epidemiological, clinical and laboratory features of leptospirosis compared to other acute febrile illnesses. J R Coll Physicians Edinb. 2020; 50 (2), 118-23.
- Kuriakose M, Eapen CK, Paul R. Leptospirosis in Kolenchery, Kerala, India: epidemiology, prevalent local serogroups and serovars and a new serovar. Eur J Epidemiol. 1997; 13 (6), 691-7.
- Clerke AM, Leuva AC, Joshi C, Trivedi SV. Clinical profile of leptospirosis in South gujarat. J Postgrad Med. 2002; 48 (2), 117-8.
- Samudyatha UC, Chaudhari V, Chauhan N, Damor R, Kosambiya JK, Munshi R. Restructuring the Modified Faine’s Criteria for the Diagnosis of Leptospirosis in Monsoon: A Study from South Gujarat. Indian J Community Med. 2020; 45 (1), 36-42.
- DebMandal M, Mandal S, Pal NK. Serologic evidence of human leptospirosis in and around Kolkata, India: a clinico-epidemiological study. Asian Pac J Trop Med. 2011; 4 (12), 1001-6.
- Karande S, Bhatt M, Kelkar A, Kulkarni M, De A, Varaiya A. An observational study to detect leptospirosis in Mumbai, India, 2000. Arch Dis Child. 2003; 88 (12), 1070-5.
- Holla R, Darshan B, Pandey L, et al. Leptospirosis in Coastal South India: A Facility Based Study. BioMed Res Int. 2018; 2018, 1759125.
- Varma MD, Vengalil S, Vallabhajosyula S, Krishnakumar PC, Vidyasagar S. Leptospirosis and dengue fever: a predictive model for early differentiation based on clinical and biochemical parameters. Trop Doct. 2014; 44 (2), 100-2.
- Gupta N, Joylin S, Ravindra P, et al. A diagnostic randomised controlled trial to study the impact of rapid diagnostic tests in patients with Acute febrile illness when compared to conventional diagnostics (DRACO study). J Infect. 2021; 82 (6), e6-e8
- Kannan A, Priya CG, Prajna L, Rathinam SR. Efficiency of two commercial kits in serodiagnosis of leptospiral uveitis. Indian J Med Microbiol. 2012; 30 (4), 418-22.
- Sharland M, Pulcini C, Harbarth S, et al. Classifying antibiotics in the WHO Essential Medicines List for optimal use-be AWaRe. Lancet Infect Dis. 2018; 18 (1), 18-20.
- Beri D, Moola S, Jagnoor J, Salam A, Bhaumik S. Prevention, control and management of leptospirosis in India: an evidence gap map. Trans R Soc Trop Med Hyg. 2021 Mar 9:trab036.
- Prahlad SR, Baxi RK, Godara N. Out-of-Pocket Expenditure and Opportunity Cost of Leptospirosis Patients at a Tertiary Care Hospital of Gujarat, India. Indian J Community Med. 2020; 45 (3), 363-6.
- Bhatt M, Soneja M, Gupta N. Approach to acute febrile illness during the COVID-19 pandemic. Drug Discov Ther. 2021; 14 (6), 282-6.
- Silva AEP, Chiaravalloti Neto F, Conceição GMS. Leptospirosis and its spatial and temporal relations with natural disasters in six municipalities of Santa Catarina, Brazil, from 2000 to 2016. Geospat Health. 2020; 26, 15(2).
- Agrawal SK, Chaudhry R, Gupta N, Arif N, Bhadur T. Decreasing trend of seroprevalence of leptospirosis at All India Institute of Medical Sciences New Delhi: 2014-2018. J Fam Med Prim Care. 2018; 7 (6), 1425-8.
- Becirovic A, Numanovic F, Dzafic F, Piljic D. Analysis of clinical and laboratory characteristics of patients with leptospirosis in five-year period. Mater socio-medica. 2020; 32 (1), 15-9.
- Everard CO, Edwards CN, Everard JD, Carrington DG. A twelve-year study of leptospirosis on Barbados. Eur J Epidemiol. 1995; 11 (3), 311-20.
- Smith S, Liu Y-H, Carter A, et al. Severe leptospirosis in tropical Australia: Optimising intensive care unit management to reduce mortality. PLoS Negl Trop Dis. 2019; 13 (12), e0007929.
- Heavy rainfall floods Udupi district; four villages inundated | Deccan Herald [Internet]. [cited 2021 the 7th of April]. Available from: https://www.deccanherald.com/state/karnataka-districts/heavy-rainfall-floods-udupi-district-four-villages-inundated-890232.html
- Temeiam N, Jareinpituk S, Phinyo P, Patumanond J, Srisawat N. Development and Validation of a simple score for diagnosis of leptospirosis at outpatient departments. PLoS Negl Trop Dis. 2020; 14 (1), e0007977.
- Chaudhry R, Batra P, Khullar S, et al. A case of neglected hepatorenal dysfunction during the COVID pandemic. Indian J Med Microbiol. 2021; 39 (2), 262-4.
- Ajjimarungsi A, Bhurayanontachai R, Chusri S. Clinical characteristics, outcomes, and predictors of leptospirosis in patients admitted to the medical intensive care unit: A retrospective analysis. J Infect Public Health. 2020; 13 (12), 2055-61.
- Biscornet L, de Comarmond J, Bibi J, Mavingui P, Dellagi K, Tortosa P, et al. An observational study of human leptospirosis in Seychelles. Am J Trop Med Hyg. 2020; 103 (3), 999-1008.
- Gkentzi D, Lagadinou M, Bountouris P, et al. Epidemiology, clinical and laboratory findings of leptospirosis in Southwestern Greece. Infect Dis Lond Engl. 2020; 52 (6), 413-8.
- Mohd Taib N, Ahmad H, Soh KL, et al. Significant clinical presentation of leptospirosis in relation to sociodemographic and risk factors in a tertiary hospital, Malaysia. Vector Borne Zoonotic Dis. 2020; 20 (4), 268-74.
- Panaphut T, Domrongkitchaiporn S, Vibhagool A, Thinkamrop B, Susaengrat W. Ceftriaxone compared with sodium penicillin g for treatment of severe leptospirosis. Clin Infect Dis. 2003; 36 (12), 1507-13.
- Raptis L, Pappas G, Akritidis N. Use of ceftriaxone in patients with severe leptospirosis. Int J Antimicrob Agents. 2006; 28 (3), 259-61.
- Sandhu RS, Ismail HB, Ja’afar MHB, Rampal S. The Predictive Factors for Severe Leptospirosis Cases in Kedah. Trop Med Infect Dis. 2020; 5 (2): 79.
- Suputtamongkol Y, Niwattayakul K, Suttinont C, et al. An open, randomized, controlled trial of penicillin, doxycycline, and cefotaxime for patients with severe leptospirosis. Clin Infect Dis. 2004; 39 (10), 1417-24.
- Costa E, Lopes AA, Sacramento E, et al. Penicillin at the late stage of leptospirosis: a randomised controlled trial. Rev Inst Med Trop Sao Paulo. 2003; 45 (3), 141-5.
- Niwattayakul K, Homvijitkul J, Niwattayakul S, Khow O, Sitprija V. Hypotension, renal failure, and pulmonary complications in leptospirosis. Ren Fail. 2002; 24 (3), 297-305.
- Philip N, Bahtiar Affendy N, Ramli SNA, et al. Leptospira interrogans and Leptospira kirschneri are the dominant Leptospira species causing human leptospirosis in Central Malaysia. PLoS Negl Trop Dis. 2020; 14 (3), e0008197.
- Daher EDF, Zanetta DMT, Abdulkader RCRM. Pattern of renal function recovery after leptospirosis acute renal failure. Nephron Clin Pract. 2004; 98 (1), c8-14.
- Johnson WD, Silva IC, Rocha H. Serum creatine phosphokinase in leptospirosis. JAMA. 1975; 233 (9), 981-2.
- Le Turnier P, Bonifay T, Mosnier E, et al. Usefulness of C-Reactive Protein in differentiating acute leptospirosis and dengue fever in French Guiana. Open Forum Infect Dis. 2019; 6 (9), ofz323.
- Crouzet J, Faucher JF, Toubin M, Hoen B, Estavoyer JM. Serum C-reactive protein (CRP) and procalcitonin (PCT) levels and kinetics in patients with leptospirosis. Eur J Clin Microbiol Infect Dis. 2011; 30 (2), 299-302.
- Fornazari F, Richini-Pereira VB, Joaquim SF, Nachtigall PG, Langoni H. Leptospirosis diagnosis among patients suspected of dengue fever in Brazil. J Venom Anim Toxins Incl Trop Dis. 2021; 27, e20200118.
- Watt G, Padre LP, Tuazon ML, et al. Placebo-controlled trial of intravenous penicillin for severe and late leptospirosis. Lancet. 1988; 1 (8583), 433-5.
- Daher EF, Nogueira CB. Evaluation of penicillin therapy in patients with leptospirosis and acute renal failure. Rev Inst Med Trop Sao Paulo. 2000; 42 (6), 327-32.
- McClain JB, Ballou WR, Harrison SM, Steinweg DL. Doxycycline therapy for leptospirosis. Ann Intern Med. 1984; 100 (5), 696-8.
- Klement-Frutos E, Tarantola A, Gourinat A-C, Floury L, Goarant C. Age-specific epidemiology of human leptospirosis in New Caledonia, 2006-2016. PloS One. 2020; 15 (11), e0242886.